
































































Respiratory Examination
Click the button to download our free OSCE Book
Introduction
- Wash Your hands
- Introduce yourself by name and Role
- Check the patient’s identity – name and Date of Birth
- Explain the procedure – why you need to do it and what does it involve
- Ask for consent
- Expose the patient appropriately
- Check if the patient is currently in any pain
How to Introduce Yourself
“Good morning, my name is .. and I am a medical student. Can I just check your name and date of birth?
I have been asked to do a respiratory examination on you, which would involve me having a look at your hands, face and chest, and then having a feel and listen to your chest. Is that ok?
– For the purposes of this examination I’m just going to position the bed at 45 degrees.
– Would you mind removing your shirt for me please?
– And can I just check whether you are in any pain?”
Bedside Inspection
- Observe the patient by standing at the end of the bed.
- Comment on whether the patient is ABC:
A – Alert B – (normal) Body habitus C – Comfortable at rest
- Observe the surroundings and comment of whether you can see any “paraphernalia of respiratory disease”:
This is a description of the objects or items around a patient’s bedside that will give you an idea into the condition that they might have. It is important to highlight this to the examiner as this can give you many clues about the patient’s underlying diagnosis. Things to look for include:
- Oxygen – is the patient currently on oxygen or room air, and what is the flow rate? Is the person on assisted ventilation.
- Inhalers – does the patient have underlying respiratory disease?
- Medication – can you see any medication on the patient’s bedside e.g. inhalers?
- Test results – are there any investigation results like CXRs or peak flow meters around the patient’s bedside.
- Fluid chart – this gives you an idea if they are fluid overloaded.
- Pillows – this is a useful marker of the level of heart failure as it shows that the patient might be suffering from orthopnoea.
- Mobility aids – gives an idea about the functional status of the patient.
Hands
Action:
Ask the Patient to put the nails of their index fingers against each other. You will be looking to see if you can detect a small rhomboid shaped window (Schamroth’s window).
Assess for:
–> Finger clubbing: this is a term which describes swelling of the distal end of the fingers which leads to loss of the angle between the nail bed and the nail. It is associated with Congenital heart disease, Infective endocarditis, Interstitial lung disease, lung cancer. BUT NOT COPD!

Action:
Ask the Patient to put their hands outstretched. Using the back of your hands, feel down from their forearms to feel the temperature:
Assess for:
–> Cold peripheries: This is a sign of poor peripheral circulation. This is a common sign of shock and so may occur in hypovolaemia when the arterioles are vasoconstricted to reduce blood supply to the extremities.
Action: Look closely at the back of the patient’s hands.
Assess for:
–> Peripheral Cyanosis: This is a blue discolouration of the nails and fingers which is indicative of peripheral ischaemia. It shows the patient is peripherally not perfusing well which can be seen in shock or hypothermia.
–> Tar staining: This is a black/brown staining of the nails and fingers which is seen in chronic smokers.
–> Koilonychia: These are spoon-shaped nails which are seen in iron-deficieny anaemia.
–> Tremor: A fine tremor in the hands is associated with beta-agonists such as salbutamol. Therefore this may be seen in asthmatic or COPD patients.


Action: Pinch the patient’s fingernail for 5 seconds and then release. Measure the capillary refill time.
Assess for:
–> Capillary refill time: This is the time taken for the capillaries to refill after a sustained period of pressure. Apply 5 seconds of pressure to the distal phalanx of the index finger and then release. Count how many seconds it taken to go red (re-vascularise). If >2 seconds, this shows poor peripheral circulation which could be a sign of shock.
Action: Ask the patient to turn their hands over and then look at the palmar surface of their hands:
Assess for:
–> Thenar eminance wasting: Wasting of the thenar muscles could be a sign of pancoast tumour, which causes compression of the lower parts of the brachial plexus which form the median nerve.
Action: Ask the patient to hold both their arms out and cock their wrists back. Ask them to keep their eyes closed and see if they can keep their hands in this position.
Assess for:
–> Asterixis: This is in ability of the patient to keep their hands cocked back. You will notice a course tremor where the hands may flap forward. This is a sign of CO2 retention and so is seen in COPD.
Wrists
Action: Feel for the Radial Pulse on one side and measure the radial pulse for 15 seconds
Assess for:
–> Rate (bpm), rhythm (regular, regularly irregular, irregularly irregular) and character (thready, bounding):
What the Radial Pulse Tells You
The radial pulse gives you a lot of information about the state of the cardiovascular system. There are 3 main variables to talk about when measuring the radial pulse:
1. Rate:
– A rate of <60bpm is considered bradycardia
– A rate of >100bpm is considered tachycardia
2. Rhythm: There are 3 main rythms to talk about:
– Regular – this will most likely be due to sinus rhythm, however you can get this in ventricular tachycardia
– Regularly irregular – this will most likely be due to a form of heart block
– Irregularly irregular – this is one not to miss and is most likely due to atrial fibrillation.
3. Character – this is gives you an indication of the strength of the impulse. It can be:
– Thready – can be seen if the BP is low such as in shock if the patient is peripherally shutting down
– Bounding – seen in CO2 retention.
Action: Feel for the radial pulse on the other side. Whilst you are feeling this, count the respiratory rate in breaths per minute. You do this by counting the number of breaths in 30s and then multiplying by 2.
Assess for:
–> Breathing rate: The normal breathing rate is 8-20 breaths per minute. Very slow or rapid breathing can lead to hypoxia and so the breathing rate is a very important variable to calculate.
Action: At this point, state that you would mention the blood pressure in both arms.
Head
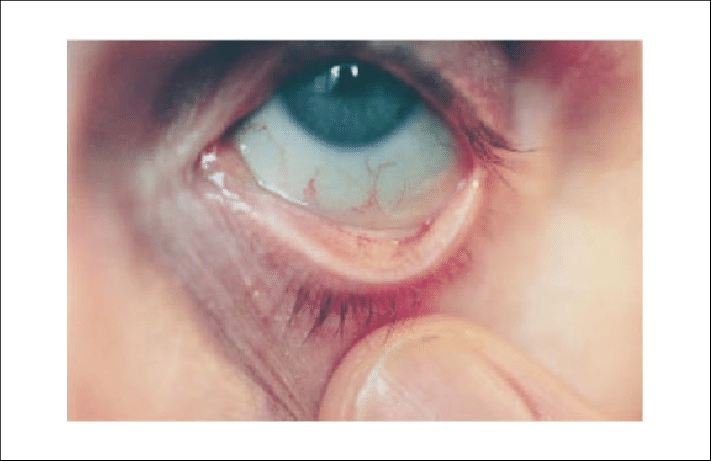
Action: Ask the patient to pull their eyelid down with their finger and look up.
Assess for:
–> Conjunctival Pallor: This is a paleness of the conjunctiva which is a sign of anaemia
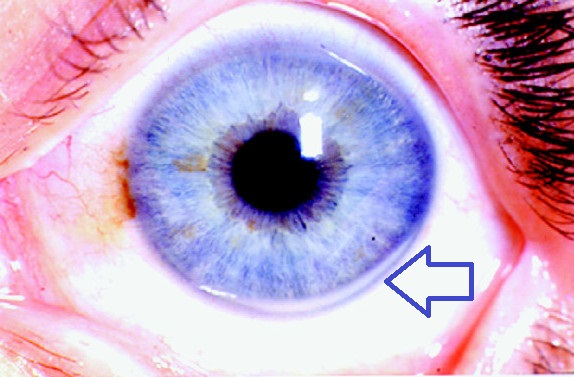
Action: Ask the patient to relax and look at their eyes.
Assess for:
–> Corneal Arcus: This is a deposit of cholesterol, phospholipids, and triglycerides in an “arc” on either the top or bottom side of the iris, which is a sign of hypercholesterolaemia. This is a risk factor for cardiovascular disease.
–> Xanthelasma: These are yellowish-white lumps of fatty material accumulated under the skin on the inner parts of your upper and lower eyelids, which are associated with hyperlipidaemia.
–> Horner’s syndrome: This is a combination of meiosis (constricted pupil), ptosis (drooping eyelid) and anhydrosis (lack of sweating). This is caused by a damage of the sympathetic fibres which supply the eye and the skin around it. There are many causes, but one not to miss is a Pancoast tumour which causes damage to the thoracic sympathetic chain in the chest. This is therefore associated with an tumour in the apex of the lungs.
Action: Ask the patient to open their mouth and stick their tongue out.
Assess for:
–> Glossitis: This is a beefy atrophic tongue which is seen in iron deficiency anaemia
–> Angular stomatitis: This is a condition that causes red, swollen patches in the corners of your mouth where your lips meet which is associated with anaemia.
Action: Ask the patient to touch the tip of their tongue to the roof of their palate. Observe the area under the tongue for blue discolouration.
Assess for:
–> Central cyanosis: This is a blue tinge of the mucosa in the mouth. This is a sign of hypoxia and will indicate that your patient is very unwell and needs urgent management.



Neck
Action: Ask the patient to relax back on the couch at 45 degrees and turn their head so they are looking left.
Assess for:
–> JVP: A raised JVP is suggestive of right heart failure, cardiac tamponade, tricuscpid regurgitation
How to Measure the JVP and Hepatojugular reflux
The internal jugular vein is runs from the middle part of the clavicle to the ear lobe. Its height above the sternal angle is a good indicate of jugular venous pressure, which indirectly measures central venous pressure.
– Usually the IJV should not be seen as right atrial pressure should be low. However in conditions like heart failure, this raises the pressure in the venous system so the internal jugular vein may become visible.
– Measure the height of the JVP by measuring the veritcle distance between the angle of the sternum and the pulsation point of the jugular vein. It should be less than 3cm
– If >3cm, this indicates that the JVP is raised and is due to conditions which stress right side of the heart
The hepatojugular reflux test
This is a test that you can do to make the IJV more visible by applying pressure to the liver. Pressing on the liver increases venous return to the heart as it is a very vascular organ. As it can cause pain, your examiner might not want you to perform this test but you should mention it to them anyways. To perform the test:
– Warn the patient that you will press on their liver quite firmly
– Apply pressure to the RUQ over their liver and observe the IJV for a rise
– A positive result is if there is a sustained rise in jugular venous pressure for more than 3cm.
Action: Check the position of the trachea. Place your index finger and your ring finger on the medial ends of both clavicles. With your middle fingers, place it on the trachea and see if it is equidistant from your two other fingers.
Assess for:
–> Tracheal deviation: A deviated trachea is associated with a pneumothorax, collapsed lung and large lesions which causes central displacement of the trachea.
Action: Check the the distance between the suprasternal notch and cricoid cartilage using your fingers.
Assess for:
–> Cricosternal distance: This is the distance between the lower border of the cricoid cartilage and the suprasternal notch. In healthy people the distance should be 3-4 fingers. If the cricosternal distance is decreased, this suggests that the lungs might be hyperinflated – therefore this is seen in obstructive conditions like COPD.
Action: Get the patient to lean forward. Stand beside them and feel the lymph nodes around their head and neck.
– Start with the submental lymph nodes –> submandibular –> pre-auricular –> posterior auricular
– Then feel the occipital lymph nodes –> supraclavicular –> infraclavicular
Assess for:
–> Lymphadenopathy: This is tender or swollen lymph nodes. This could be a sign of cancer or a respiratory tract infection.
Chest
OBSERVE
Action: Ask patient to put their hands on hips so that you can view their axilla. Have a good look all around for any potential scars or chest wall deformities.
Assess for:
–> Chest Wall Deformities:
- Pectus excavatum: This is a sunken appearance of the chest, which can be seen in Marfan’s syndrome
- Pectus carinatum: This is when the chest sternum bulges from the chest
–> Scars:
- Lateral thoracotomy scar – may indicate previous mitral valvotomy
- Axillary thoracotomy scar – This scar will be in line between the posterior border of the pectoralis major and anterior border of latissimus dorsi muscles. It is used for the insertion of chest drains
- Posterolateral thoracotomy scar – site for pacemaker



PALPATE
Action: Find apex beat – 5th intercostal space in left mid-clavicular line
Assess for:
–> Apex beat displacement: If the apex beat is displaced, this can be a sign of cardiomegaly due to ventricular hypertrophy. It can also be due to a tension pneumothorax or a space occupying lesion.
Action: Place your hand on the patient’s chest parallel to the left sternal edge.
Assess for:
–> Heaves – This is a contraction impulse that can be felt by your hand and it is a sign of right sided ventricular hypertrophy. If heaves are present then you will be able to feel an upward force of your hand
Action: Place your hands over the patient’s chest on their pectoral muscles and wrap your fingers around their chest.
– When the patient breathes out, bring your two thumbs together in the midline
– Ask the patient to take a deep breath in. Observe how your two hands are pushed outwards as the chest expands.
– Repeat this procedure at the subcostal margin.
Assess for:
–> Bilateral chest wall expansion: You should see both your thumbs move outwards by the same amount. This shows the lungs have bilateral chest expansion. You may notice symmterical or asymmetrical poor chest expansion:
– Asymetrical lung expansion – Pneumonia, pneumothorax
– Symmeterical lung expansion – Restrictive pathologies e.g. interstitial lung disease, motor neurone disease
PERCUSS
Action: Percuss the lungs from the front to assess for resonance.
– In order to percuss, place your middle finger of your non-dominant hand on the patient’s chest
– With your middle fingers of your dominant hand, tap down on the other middle finger using a bouncing motion
– Start with the apices of both lungs, and move down and across the lungs
Assess for:
–> Resonance beat: If the lungs are full of air they should sound resonant to percussion. On the other hand, hyper-resonance (too much air) or stony dullness (due to consolidation or pleural effusion) is indicative of a lung pathology.
AUSCULTATE
Action: Using your stethoscope, have a listen to the various zones of the lung (12)
- Lung apices – Listen to these will the bell of the stethoscope
- Infraclavicular region – ajacent to second costal cartilage
- Chest wall – go down every 2-3 costal cartilages
- Lung bases – right on the subcostal margin

Assess for:
–> Breath sounds: This is to hear the amplitude and quality of the breath sounds from the lungs. An increase in resitance, consolidation or blockage all provide very different sounds which it is important to be able to differentiate.
Types of Breath Sounds
Vesicular: normal breath sounds which are heard usually
Bronchial breathing: this is a harsh sounding movement of air which is due to the sound of air in the bronchioles. This is a sign of consolidation as you usually should not be able to hear air movement here.
Wheeze: this is a a horn like sound which is associated with obstructive conditions like asthma and COPD
Inspiratory Stridor: this is a high-pitched breath sound which is indicative of upper airway obstruction
Coarse crackles: these are popping breathing sounds which are associated with consolidation in the lungs
Fine end-inspiratory crackles: these sound like stepping on snow. They are associated with interstitial lung disease and pulmonary fibrosis.
RE-PERCUSS AND AUSCULTATE ON BACK
Action: Ask the patient to lean over and cross their arms. Move around to the patient’s back and repeat the percussion and auscultation this time from the patient’s back.
VOCAL RESONANCE
Action: Ask the patient to lean forward. Place your stethoscope over the auscultation points on their back.
– This time, get the patient to say the words “Ninety-nine” when you place the stethoscope on their back.
Assess for:
–> Vocal Resonance: This is a measure of how well the underlying tissue is able to conduct the sound waves to your stethoscope. This will depend on factors such as whether there is more tissue density or volume.
– Increased vocal resonance – increase in tissue density e.g. tumour, consolidation
– Decreased vocal resonance – decrease in tissue density e.g. asthma, COPD, pneumothorax, pleural effusion
Action: Whilst the patient is leaning forward, feel their sacrum
Assess for:
–> Sacral oedema: This is a sign of peripheral oedema which is associated with right-sided heart failure.
Legs
Action: Ask the patient to keep their legs outstretched. Closely inspect their feet and legs for any signs of cardiovascular disease.
Assess for:
–> Scars: Look for vein harvesting scars for a CABG. The great saphenous vein is often used as the graft for a coronary bypass surgery, so this will indicate that the patient has ischaemic disease.
–> Varicose veins: These are dilated and tortuous veins secondary to chronic venous insufficiency
–> Calf Tenderness: A red swollen or tender calf unilaterally is a sign of a deep vein thrombosis. This needs urgent assessment with ultrasound as the patient is at high risk for a pulmonary embolus.
Action: Press on the medial malleolus of the patient ankles and assess if you can see/feel any sinking of the skin and whether it takes long to rise back up. If positive, see how far up the legs this oedema goes.
Assess for:
–> Pitting oedema: This is a sign that the patient is fluid overloaded. It is associated with right sided heart failure but can also be seen in conditions which reduce oncotic pressure e.g. hepatic failure.


Thank the patient and wash your hands to complete the examination!
On Completion
You must remember that the physical examination is only one part of the overall assessment of your patient. Therefore, when completing your exam, state that you would do the following in order to complete your assessment of the patient. Much of this will depend on whether you have discovered any particular findings or have an idea about the overall diagnosis. However, some essential things to talk about are:
“To complete the examination, I would do a number of steps…”
Bedside – (History) Take a full history
- (Observations) Full set of observations chart including blood pressure and SpO2.
- (Corresponding examination) Conduct a cardiovascular examination
- (Bedside tests) Take a peak flow and sputum culture and spirometry
Bloods – Would take a full blood count, U&Es and inflammatory markers
Imaging – Chest X-ray
Special tests – CT chest (if required)
How to Present Your Findings
“I conducted a respiratory examination on … who seemed well and comfortable at rest.
- On inspection there were no peripheral signs of respiratory disease and no paraphernalia of respiratory disease.
- They had a pulse rate of … and a breathing rate of ….. Their pulse was regular and character normal
- The JVP was (3)cm so not raised.
- There was bilateral chest expansion and no tracheal deviation.
- On percussion, the lungs were resonant bilaterally.
- On auscultation there were vesicular breath sounds throughout.
- There was no pitting oedema and the calves were soft and non-tender.added sounds, and lung bases clear bilaterally.
In summary, this is a normal examination.”
Sources
Finger Clubbing – Desherinka, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Tar Staining – James Heilman, MD, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Koilonychia – CHeitz, CC BY 2.0 <https://creativecommons.org/licenses/by/2.0>, via Wikimedia Commons
Conjunctival Pallor – Sheth TN, Detsky AS. The relation of conjunctival pallor to the presence of anemia. J Gen Intern Med. 1997;12(2):102-106.
Corneal Arcus – Loren A Zech Jr and Jeffery M Hoeg, CC BY 2.0 <https://creativecommons.org/licenses/by/2.0>, via Wikimedia Commons
Xanthelasma – Klaus D. Peter, Wiehl, Germany, CC BY 3.0 DE <https://creativecommons.org/licenses/by/3.0/de/deed.en>, via Wikimedia Commons
Glossitis – Martin Kronawitter, CC BY-SA 2.5 <https://creativecommons.org/licenses/by-sa/2.5>, via Wikimedia Commons
Angular Stomatitis – Matthew Ferguson 57, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Pectus Excavatum – From Wikimedia Commons, the free media repository
Pectus Carinatum – Jprealini, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Median Sternotomy – Stockholm, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Lung Markings – Surface Anatomy, 4 Edition Chapter 4. Thorax
Varicose Veins – self, Public domain, via Wikimedia Commons
Pitting oedema – James Heilman, MD, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Disclaimer
The intended purpose of this website is to be used as a resource for revision for exams. It should not be used as a guideline or reference for clinical practice/decision making or by patients looking for medical information or advice. In2Med takes no responsibility for any loss or damaged resulting from the use of information from this website.


