
































































Hip Examination
Click the button to download our free OSCE Book
Introduction
- Wash Your hands
- Introduce yourself by name and role
- Check the patient’s identity – name and Date of Birth
- Explain the procedure – why you need to do it and what does it involve
- Ask for consent
- Expose the patient appropriately
- Check if the patient is currently in any pain
How to Introduce Yourself
“Good morning, my name is .. and I am a medical student. Can I just check your name and date of birth?
-I have been asked to do an examination on your hip. This will involve me asking you to walk and then having a look, feel and moving the hip joint. Is that ok?
– For the purposes of this examination would you mind removing your trousers but keeping your underwear on?
– And before I start can I just check whether you are in any pain?”
Bedside Inspection
- Observe the patient by standing at the end of the bed.
- Comment on whether the patient is ABC:
A – Alert B – (normal) Body habitus C – Comfortable at rest
- Observe the surroundings and comment of whether you can see any “paraphernalia of musculoskeletal disease”:
This is a description of the objects or items around a patient’s bedside that will give you an idea into the condition that they might have. It is important to highlight this to the examiner as this can give you many clues about the patient’s underlying diagnosis. Things to look for include:
- Hands – the patient’s hands may indicate osteoarthritis or rheumatoid arthritis.
- Mobility aids/Zimmer frames, shoes (heel raises and supports) – gives an idea about the functional status of the patient.
- Medication– any pain relief or steroids at the bedside?
Gait
Action: Ask the patient to walk to the end of the room, turn around and then walk back.
Assess for:
–> Smoothness: Is there any disruption to the normal gait cycle such as abnormalities in toe-off or heel strike?
–> Symmetry: Is the gait symmetrical on both sides? Asymmetry of the gait could be caused by problems such as leg-length discrepancy, fixed flexion deformity, or pain on one side which reduces full extension and weight bearing on that side.
–> Step Height: A damage to the common fibular nerve for example leads to a foot-drop on the affected side. This means the patient will not be able to dorsiflex which gives them a high step height to compensate.

Types of Gait
The gait cycle is made up of 6 phases.
- Heel-strike: this is when the heel first touches the floor.
- Foot flat: here the weight is transferred onto the leg as the foot is all in contact with the floor.
- Mid-stance: the weight is aligned and balanced on this leg.
- Heel-off: here the heel lifts off as you start to transfer weight onto the other leg.
- Toe-off: this is when the toes finally lift off the floor
- Swing: the foot swings forward until the heel comes back in contact with the ground restarting the cycle.
a) Antalgic gait – a type of gait where the stance phase is abnormally shortened to reduce time on that foot. It looks like a limp –> implies pain in that leg
b) Waddling gait – this is due to weakness of the proximal muscles of pelvis which causes weakness of gluteus muscles. Patient moves upper body forwards and drags lower leg forward.
c) Spastic gait – this is described as a swinging gait where the patient swings his leg round as it is hyperextended. This is seen in UMN lesions such as stroke
d) High-stepping gait – this is due to damage of the deep branch of the common fibular nerve which leads to foot-drop due to loss of dorsiflexion. This means the patient has a high step in order to compensate.
e) Trendelenburg gait – this leads to dropping of the pelvis on the contralateral side when you are walking. It is due to damage to the gluteus medius on the supported side –> indicates a lesion of the superior gluteal nerve
f) Fixed flexion/hyperextended knee– the knee is in fixed flexion/knee is hyperextended- occurs in polio as patient have quadriceps wasting
Observation – Standing
Action: Ask the patient to stand upright with their arms by their side. Observe them from the front, side and back for any signs of musculoskeletal disease.
FROM THE FRONT:
Assess for:
–> Scars: These are indicators of any previous surgery, such as a hemiarthroplasty or a total hip replacement.
–> Pelvic tilt: This is asymmetry of the pelvic girdle. A pelvic tilt may indicate weakness of the abductor muscles e.g. gluteus medius due to damage to the superior rectal nerve.
–> Asymmetry/leg length discrepancy: Leg length discrepancy could be due to joint disease as a child, or a fixed flexion deformity of one of the limbs.
–> Quadriceps: Assess for any wasting of the quadriceps muscle bulk. This could be due to damage to the femoral nerve, but it also occurs after surgery due to inactivity and wasting of the quadriceps muscles.

FROM THE SIDE:
Assess for:
–> Spine: Assess for loss of lumbar lordosis which could indicate a fixed flexion deformity.
–> Foot arches: Flattening of the feet or high arched feet are associated with condition. A high arch (pes cavus) is seen in Charcot-Marie-Tooth disease. Flat feet (pes planus) are risk factors for joint problems.
FROM THE BACK:
Assess for:
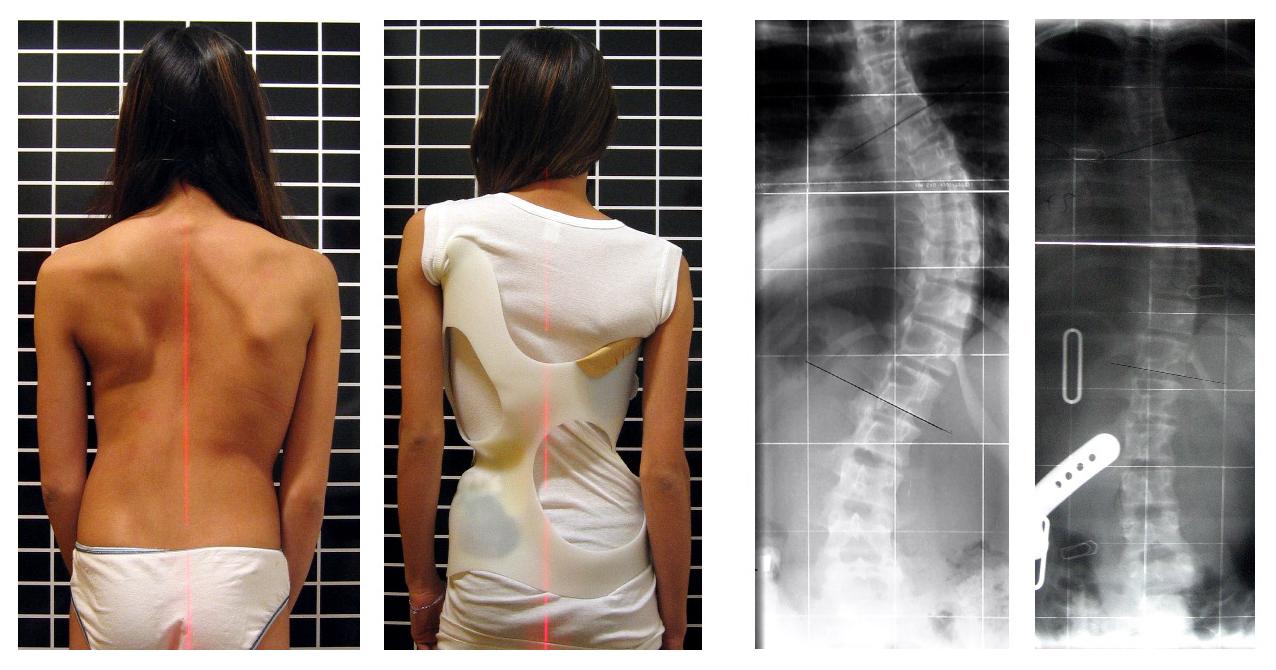
–> Scoliosis: This is a lateral curvature of the spine which is more common in adolescent girls. If severe, this may require surgery to correct the spine.
–> Gluteal wasting: This is wasting of the gluteal muscles which form the buttocks.
–> Asymmetry of pelvic brim: Similar to assessing from the front, you can use the “Dimples of Venus” to assess for assymetry of the pelvic girdle from the back. These are sagittal symmetrical indentations sometimes visible on the human lower back, just superior to the gluteal cleft. These indentations are created by a short ligament stretching between the posterior superior iliac spine and the skin.



Trendelenburg’s Test
This is a test which is used to assess for weakness in the hip abductor muscles, gluteus medius and minimus.
Action: Perform Trendelenburg’s test on the patient.
a. With the patient standing, stand behind the patient so you can clearly see their pelvis.
b. Ask the patient to lift one foot off the floor by flexing their hip and knee on that side. Ask them to hold this position for 10 seconds.
c. Observe what happens to the pelvic girdle.
d. Repeat the assessment with the other side.
Assess for:
–> Dropping of the pelvis: In a healthy patient, the hip abductors on the side of the leg which is standing contract to shift the centre of gravity to the standing leg and keeping the pelvic girdle level. This gives stability to the patient.
– What you might find is that the pelvis drops on the side of the raised leg. This is due to weakness of the contralateral abductor muscles on the side of the standing leg.

Observation- lying
Action: Ask the patient to lay down on the couch with the seat reclined at 45 degrees. Tell them to keep their legs outstretched and relaxed so that you can inspect their legs.
Assess for:
–> Scars: Have a closer look for any scars indicative of previous hip surgery.
–> Muscles: Compare both sides looking for evidence of muscle wasting or fasciculations.
–> Abnormal positions: Look at the resting angle of the legs. Are they abducted, externally rotated or is there any evidence of limb shortening?


Leg lengths
Action: Offer to measure the true and apparent leg length. In your exam, the examiner may give you a measuring tape so you can formally assess this:
Assess for:
–> Apparent leg length: This is measured from the umbilicus to the medial malleolus. A discrepancy in the apparent leg length is suggestive of a tilted pelvis, which makes the legs appear unequal in length. This is often due to spinal or pelvic problems e.g. scoliosis.
–> True leg length: This is measures from the ASIS to the ipsilateral medial malleolus. Unequal true leg lengths is more suggestive of an actual limb pathology which leads to shortening e.g. neck of femur fracture.
Feel
Action: With the patient lying down, using the backs of your hands, palpate both the hip joints, seeing if you can find a temperature difference between the two legs.
Assess for:
–> Temperature: A raised temperature is indicative of an inflammatory process occurring. This could be due to an inflammatory arthritis e.g. rheumatoid arthritis, septic arthritis.
Action: Palpate the hip joints, starting with the normal side first and then moving onto the side which is giving the patient trouble.
a. Start medially at the pubic symphysis.
b. Work round laterally across the anterior aspect of the hip joint.
c. When you are at the side, move your fingers inferiorly so you can palpate the greater trochanter.
d. Complete by palpating round the posterior aspect of the hip join.
Assess for:
–> Tenderness: This may indicate an inflammatory process or something more acute like a fracture. It is important to localise the tenderness as different pathologies give pain in different areas.
–> Trochanteric bursitis: This is inflammation of the bursa over the greater trochanter. It will be detected by focal tenderness over the trochanter.

Move
In the MSK examinations, we assess both active (patient doing the movement unaided) and passive movement (where the examiner does the movement for them). This is because different pathologies will produce pain on active or passive movement, or sometimes both. This is crucial in helping the clinician to diagnose the condition.
–> Pain on active movement – Tendon issues, muscle conditions
–> Pain on passive and active movement – Joint conditions, fractures
ACTIVE MOVEMENT:
Action: To test the movements, make the bed completely flat to allow for a full ROM. Test each leg in turn.
a. Hip Flexion: Ask patient to bring their knee towards chest. (Normal ROM is 120 degrees)
PASSIVE MOVEMENT:
This time, ask the patient to relax and allow you to move the joint freely. To help achieve this, start by rolling each leg side to side gently to make the leg floppy. When doing passive movement, keep one hand on the hip so you can feel for any crepitus in the joint.
Actions:
a. Hip flexion: Support the leg and flex the hip bringing the knee towards the patient’s chest. (Normal ROM is 120 degrees)
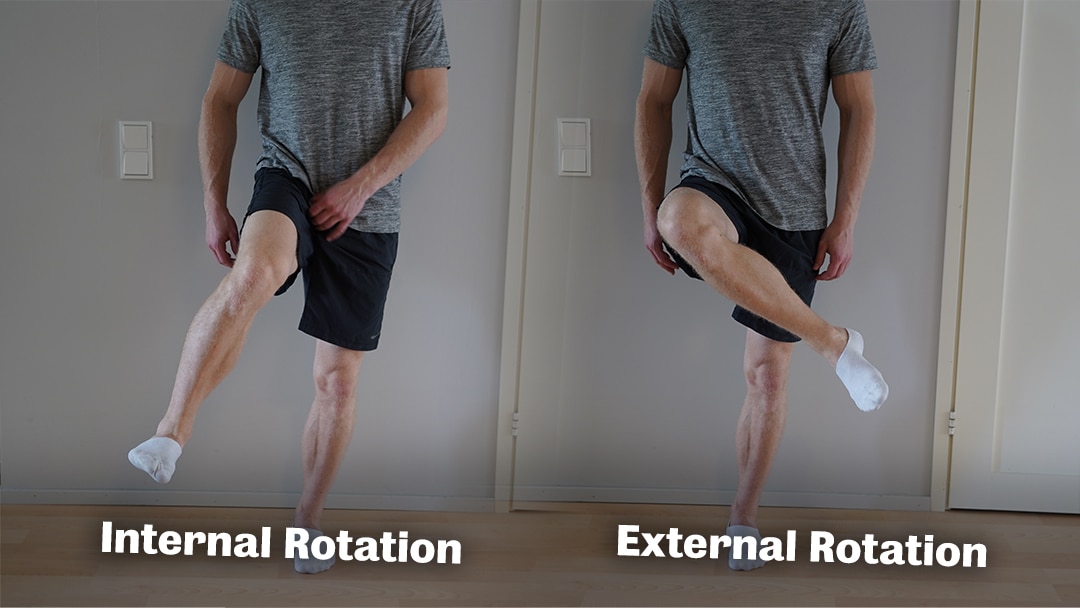
b. Internal and External Rotation: Whilst the hip is flexed to 90 degrees, turn the knee inwards to internally rotate the hip (Normal ROM = 30 degrees) and then outwards to externally rotate the hip (normal ROM = 40 degrees)
c. Abduction and Adduction: Place your left hand on contralateral iliac crest to detect pelvic movement. Hold calf in right hand and abduct the hip by moving the calf outwards (normal ROM = 45 degrees). Then test adduction by crossing leg over the other one.
Bring the leg back to its original position and repeat on other leg.
d. Passive Extension: Ask the patient to turn over so that they are lying on their front. Hold the leg by the calf and lift it up to passively extend the hip, one leg at a time. (Normal ROM = 10-20 degrees)
Assess for:
–> Crepitus: This is a sensation or noise when you move a joint which can be described as clicking, cracking, creaking, crunching, grating or popping. The sound is heard when two rough surfaces come into contact—for example, in osteoarthritis or rheumatoid arthritis when the cartilage around joints erodes and the surfaces in the joint grind against one another. Therefore, could be a sign of arthritis in the hip joint.
–> Range of Motion: For each movement, assess whether the patient has a normal range of motion. When assessing this, try and distinguish whether this the ROM is limited due to a structural abnormality or pain.
Special tests
Thomas’ Test:
This is a test which is used to assess for a fixed flexion deformity in the legs. You may have already detected this earlier in your examination, but this test is more sensitive at detecting it. You must perform this test with caution as it can cause a hip dislocation in patients with hip replacement. Therefore, it is important to ask the patient before you do this test – or at least mention this to your examiner.
Action: Perform Thomas’ test on the patient.
a. With the bed fully flat, ask the patient to lay with their legs outstretched fully relaxed.
b. Place your left hand under their lumbar spine with palm facing upwards. You may detect some lumbar lordosis.
c. Ask the patient to bring both knees to their chest. The lumbar lordosis will flatten
d. Ask the patient to straighten each of their legs one after the other. Observe what happens to the contralateral leg.
Assess for:
–> Fixed flexion deformity: In a healthy patient, they should be able to extend both legs fully.
– If there is a fixed flexion deformity, they will be unable to full extend that leg whilst the other one is flexed.
– The patient may compensate for the deformity with increased lumbar lordosis. Here, you will notice that the lumbar spine lifts off from your hand. This should therefore be regarded as a positive result as shows there is a fixed flexion deformity in that leg.

Thank the patient and wash your hands again!
On Completion
You must remember that the physical examination is only one part of the overall assessment of your patient. Therefore, when completing your exam, state that you would do the following in order to complete your assessment of the patient. Much of this will depend on whether you have discovered any particular findings or have an idea about the overall diagnosis. However, some essential things to talk about are:
“To complete the examination, I would do a number of steps…”
Bedside:
- (History) Take a full history
- (Observations) Examine neurovascular state of both limbs e.g. pulse, sensation, proprioception
- (Corresponding examination) Examine joint above and below (knee and spine)
- Check for the presence of hernias – these give atypical groin/hip pain
Bloods – Would take a full blood count, inflammatory markers
Imaging – AP and lateral radiographs of the knees and hip
How to Present Your Findings
“I conducted a hip examination on … who seemed well and comfortable at rest.
- On inspection there were no peripheral signs or paraphernalia of MSK disease
- The gait was smooth with a normal swing and stance phase
- There was normal range of active and passive motion in the hips
- There was no evidence of pelvic tilt or fixed flexion deformity of the hip
- There was no tenderness over the greater trochanter
In summary, this is a normal examination.”
Sources
Gait Cycle – Ducky2315, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Pelvic Tilt – See page for author, CC BY 2.0 <https://creativecommons.org/licenses/by/2.0>, via Wikimedia Commons
Pes Planus – Hellerhoff, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Pes Cavus – Benefros at English Wikipedia, CC BY-SA 3.0 <http://creativecommons.org/licenses/by-sa/3.0/>, via Wikimedia Commons
Scoliosis – Weiss HR, CC BY 2.0 <https://creativecommons.org/licenses/by/2.0>, via Wikimedia Commons
Dimples of Venus – Piotr from Poznań, Poland, CC BY-SA 2.0 <https://creativecommons.org/licenses/by-sa/2.0>, via Wikimedia Commons
Trendelenburg Sign – S. Bhimji, CC BY 4.0 <https://creativecommons.org/licenses/by/4.0>, via Wikimedia Commons
Hip Replacement Scar – Karl-Heinz Wellmann, CC BY 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons
Hip Fracture – DocP at German Wikipedia, CC BY-SA 3.0 DE <https://creativecommons.org/licenses/by-sa/3.0/de/deed.en>, via Wikimedia Commons
Hip Anatomy – BruceBlaus, CC BY 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons
Hip Flexion – Mapommered, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Hip internal and external rotation – https://vahvafitness.com/unilateral-hip-rotation-for-maximal-performance/
Hip abduction – SportEX Journal, Hip abduction assisted exercise using turbulence, Attribution-NoDerivs 2.0 Generic (CC BY-ND 2.0)
Thomas’ Test – Reliability of the Thomas test for assessing range of motion about the hip – Scientific Figure on ResearchGate. Available from: https://www.researchgate.net/figure/Thomas-Test-visual-representation-of-pass-fail-scoring-a-Pass-score-participants_fig1_229071146
Disclaimer
The intended purpose of this website is to be used as a resource for revision for exams. It should not be used as a guideline or reference for clinical practice/decision making or by patients looking for medical information or advice. In2Med takes no responsibility for any loss or damaged resulting from the use of information from this website.


