
































































Parkinson’s examination
Click the button to download our free OSCE Book
Summary
Parkinson’s is a disease where the dopaminergic neurones in the substantia nigra are progressively lost.
– This leads to excessive filtering due to a weak direct pathway restricting voluntary movements.
– Can be drug-induced – gives motor symptoms rapid onset and bilateral with a faster onset
The key symptoms of Parkinson’s can be grouped into a triad:
1) Tremor –> worse at rest (pill rolling motion of thumb over fingers), improves with movement
2) Hypertonia –> cogwheel rigidity in the extremities
3) Bradykinesia –> slow initiation of voluntary movements and expressionless face (Mask face)
– Postural instability and shuffling gait –> festinant (shuffling, pitched forward gait)
– Also occurs with depression (most common mental symptom), dementia and psychosis
These are the main symptoms that we assess for in a focussed Parkinson’s examination.
Introduction
- Wash Your hands
- Introduce yourself by name and Role
- Check the patient’s identity – name and Date of Birth
- Explain the procedure – why you need to do it and what does it involve
- Ask for consent
- Expose the patient appropriately
- Check if the patient is currently in any pain
How to Introduce Yourself
“Good morning, my name is .. and I am a medical student. Can I just check your name and date of birth?
I have been asked to do a neurological examination. This will involve asking you some questions, and assessing the tone and movements of your arms and legs. Is that ok?
Can I first check whether you are in any pain?”
Focused questions
Whilst it is unlikely you will have time to ask these questions in an OSCE, to get an overall sense of the condition in clinical practice, you may want to ask these 3 questions to give you more information about the patient’s condition.
Q1) What happened when you first presented with this condition? How is it affecting you?
Q2) When is your tremor worst?
Q3) Do you have any problems with: balance, co-ordination, doing up buttons and tying shoelaces, getting in and out of your car?
Bedside Inspection
- Observe the patient by standing at the end of the bed.
- Comment on whether the patient is ABC:
A – Alert B – (normal) Body habitus C – Comfortable at rest
- Assess for abnormal posture and scars.
- Do they have a resting tremor?
- Observe the surroundings and comment of whether you can see any “paraphernalia of neurological disease”:
This is a description of the objects or items around a patient’s bedside that will give you an idea into the condition that they might have. It is important to highlight this to the examiner as this can give you many clues about the patient’s underlying diagnosis. Things to look for include:
- Mobility and hearing aids – gives an idea about the functional status of the patient.
- Medications– iatrogenic causes of cerebellar signs eg phenytoin or medications related to ischaemic vascular disease or thyroid disease.
- Test results – are there any investigation results around the patient’s bedside.
Gait
Action: Ask patient to stand up with arms folded
Assess for:
–> Proximal Muscle Weakness. This could be due to a myopathy which leads to weakness of the main extensors of the trunk, leading to an inability to stand from a seated position.
Action: Ask the patient to walk to the end of the room, turn around and then walk back.
Assess for:
–> Smoothness: Is there any disruption to the normal gait cycle such as abnormalities in toe-off or heel strike?
–> Symmetry: Is the gait symmetrical on both sides? Asymmetry of the gait could be caused by problems such as leg-length discrepancy, fixed flexion deformity, or pain on one side which reduces full extension and weight bearing on that side.
–> Step Height: A damage to the common fibular nerve for example leads to a foot-drop on the affected side. This means the patient will not be able to dorsiflex which gives them a high step height to compensate.

Gait Changes in Parkinson's Disease
Face
Action: Take a look at the patient’s face the patient’s face
Assess for:
–> Hypomimia: This refers to reduced facial expressions. Patient with Parkinson’s exhibit a “mask-like” face which is not expressive with a reduced frequency of blinking. It occurs due to motor impairment of the facial muscles due to the loss of dopamine in the basal ganglia.

Action: Ask the patient to describe the room around them in order to test their speech.
Assess for:
–> Hypophonia: This is the tendency to speak softly, generally as a result of impairments in the muscles that are used to form speech. This can make the speech very faint and difficult to understand, which is why patients with PD exhibit difficulties in communication.
Glabellar Tap
Action: Perform the Glabellar reflex:
a. Ask the patient to look at you
b. Tap the patient repeatedly on the glabella — this is the smooth part of the forehead above the nose and between the eyebrows of the patient
c. Observe the patient’s eyes to see if they start blinking
Assess for:
–> Myerson’s sign: In a healthy patient, the eyes will start blinking by reflex when you tap their forehead. But after a few seconds the body will habituate and they will stop. This is because it is a primitive reflex which is seen in babies, but adults do not exhibit this as their frontal lobe develops. In Parkinson’s patients, the blinking reflex often persists with the tapping. This is known as Myerson’s sign and it is due to frontal lobe release.
Tremors
A characteristic sign of Parkinson’s disease is the presences of tremors. However, it is important to know that there is more than one type of tremor – in addition, just because a patient has a tremor does not mean that they have PD. We aim to assess for 3 types of tremors in the Parkinson’s examination.
Pill-rolling (resting) Tremor
Action: Ask the patient to sit and relax their arms and observe them. You can test for this tremor earlier in your exam when you are doing your general inspection rather than just asking the patient to sit relaxed. However, you must not miss it out in your exam.
Assess for:
–> Resting tremor: This is a characteristic sign which is usually asymmetrical (in one hand only). It is described as “pill-rolling” as the tremor resembles someone rolling a tablet in their hands. It is usually 4-6Hz in amplitude.
Postural tremor
Action: Ask patient to hold out their arms fully extended in front of their body with their palms facing down.
Assess for:
–> Postural tremor: This is a type of tremor that occurs when the patient is trying to maintain a position against gravity. This tremor worsens during the movement.

Kinetic tremor
Action: Get the patient to perform the finger nose test
a. Tell the patient to touch their nose with their index finger
b. Now place your finger in front of the patient in a position whether they could stretch their arm to touch it
c. Ask the patient to now touch your finger
d. Ask the patient to touch their nose again and repeat the cycle 3 times. Each time, move your own finger to a new position.
Assess for:
–> Simple Kinetic tremor: This is a type of tremor that occurs during hand movements. In this tremor, it will remain a constant amplitude during the whole movement. when the patient is trying to maintain a position against gravity. This tremor worsens during the movement.
–> Intention Tremor: This is a type of kinetic tremor which will get more intense as the patient nears the target (your finger). It is a sign of cerebellar dysfunction.

Focussed Upper Limb
TONE
Testing the tone is an essential part in helping to distinguish whether the nerve lesion is upper or lower. Upper motor neurone lesions typically give hypertonia, whereas lower motor neurone lesions give reduced muscle tone.
Action: Ask the patient to fully relax their muscles so you can passively move them. Support their elbow with one hand and with the other hand hold their hand like you are giving them a handshake.
– Shoulder: Extend and flex the shoulder moving the arm towards you and away.
– Elbow: Support the elbow and holding the hand, carry out passive flexion and extension of the elbow.
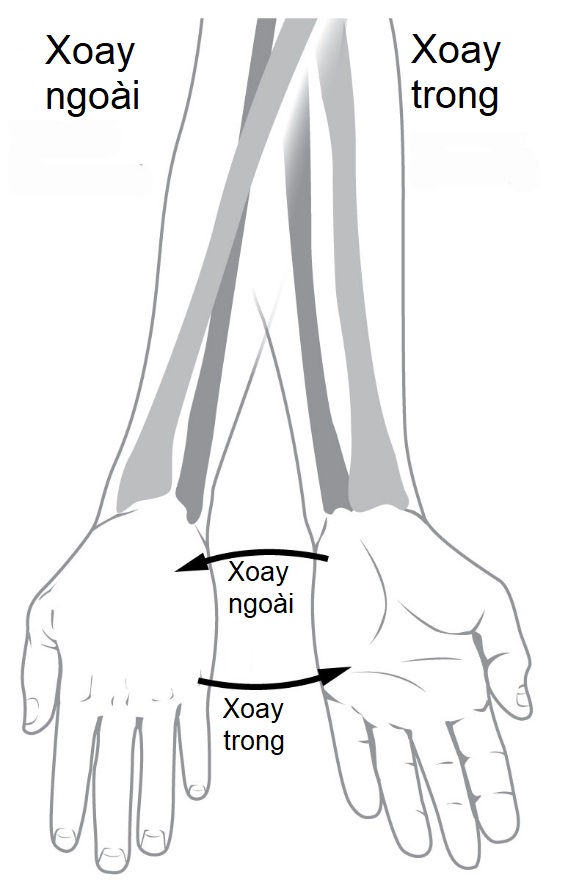
– Forearm: In same position, with the elbow at 90-degree flexion, pronate and supinate. Repeat this movement again supinating the forearm very quickly to assess for supinator catch.
– Wrist: Ask the patient to make a fist. Hold their fist and use it to flex/extend and rotate the wrist.
Assess for:
–> Hypo/hypertonia: Hypotonia is associated with LMN lesions and hypertonia with UMN lesions.
–> Supinator catch: When supinating the forearm, this is a brief “catch” that you will feel in the movement as you rotate. It is associated with spasticity and so is a UMN sign.
–> Cogwheel rigidity: This is a clinical sign associated with Parkinson’s disease. Here the muscle will move and then get stuck intermittently like a cogwheel. It is velocity independent, meaning it is the same whether you move the muscle quickly or slowly.
–> Leadpipe rigidity: This is a clinical sign where there is increased tone throughout the whole movement of the muscle. It feels like you are trying to move a lead-pipe which is very stiff. It is “velocity-independent” meaning that it is the same whether you move the muscle quickly or slowly. It is seen in neuroleptic malignant syndrome.
BRADYKINESIA
Bradykinesia is a characteristic symptom in Parkinson’s disease which refers to slowness in the initiation of movement. In order to assess for bradykinesia in the upper limb, we test 3 specific movements.
Action: Ask the patient to do these 3 movements. Test the left and the right side separately:
a) Wrist: Ask the patient to supinate and then pronate their wrist repeatedly as fast as they can for 10 seconds.
b) Hand: Ask the patient to make a fist with their hand and then open it up repeatedly as many times as they can in 10 seconds.
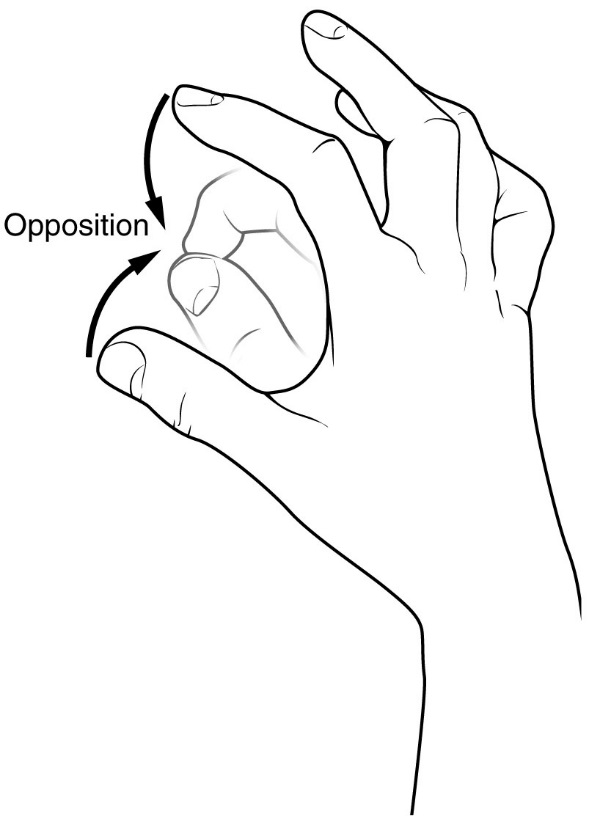
c) Fingers: Ask the patient to touch the index finger to their thumb as fast as they can repeatedly for 10s.
Assess for:
–> Bradykinesia: This is a characteristic sign of PD. Patient will exhibit slowness in initiating the movement and over time you may see a reduction in the speed and amplitude of the movement. A key sign is that it affects the limbs asymmetrically, so observe for differences between the right and left hands.

Focussed Lower Limb
In the parkinson’s examination, it is important to assess for bradykinesia in the legs as well as the arm.
Toe Tap:
Action: Ask the patient
Assess for:
–> Bradykinesia: This is a slowness in the initiation of movement and freezing, which occurs due to loss of dopamine in the basal gangle.

Extras
Once you have covered the core elements fo the Parkinson’s examination, you may also want to assess for extra features to gain a more comprehensive understanding of the patient’s condition and functional status.
Action: Ask the patient to copy a sentence and look at their handwriting.
Assess for:
–> Asymmetric progressive micrographia: Micrographia is abnormally small or cramped handwriting. It is a secondary motor symptom experienced by some people with Parkinson’s disease (PD). Micrographia is believed to be a result of bradykinesia, the slowing down and loss of spontaneous movement

Action: Ask the patient to
Assess for:
–> Dexterity: Parkinson’s patients will find this task difficult due to the bradykinesia which limits dexterity in doing tasks which require intricate movements.
This refers to some conditions which exhibit Parkinson’s-like symptoms, due to the loss of dopamine in the substantia nigra which slows down voluntary movement. However, in these conditions, other organs/tissues are also affected which give additional symptoms. You will not be expected to test for these in your OSCE, but you may get asked questions about them.
One of the best ways to screen for these symptoms is to examine the eye movements.
Action: Perform the H-test to assess the motor function of the extra-ocular muscles.
a. Sit opposite the patient and hold your finger up in front of the patient’s eyes. Ask the patient to focus on your finger.
b. You can use your other hand to support the top of the patient’s head to ensure that the head stays still.
c. Ask the patient to follow your finger with their eyes, ensuring they keep their head still.
d. Move your finger from side to side, then up and down creating a big “H” pattern.
Assess for:
–-> Progressive Supranuclear Palsy: This is a condition which affects multiple parts of the brain. The basal ganglia are affected giving rise to the Parkinsonism, but also the tectum which controls the eye movements. In addition it affects the cerebellum, spinal cord and the limbic system. In the “H” test, the patient may show difficulty in looking up.
–> Multisystem atrophy: This is a is a rare neurodegenerative disorder which gives the Parkinsonism features. However, it is characterised by autonomic dysfunction (e.g. hypotension) and damage to the cerebellum which leads to ataxia. Therefore, in the “H” test the patient may show nystagmus.
On Completion
You must remember that the physical examination is only one part of the overall assessment of your patient. Therefore, when completing your exam, state that you would do the following in order to complete your assessment of the patient. Much of this will depend on whether you have discovered any particular findings or have an idea about the overall diagnosis. However, some essential things to talk about are:
“To complete the examination, I would do a number of steps…”
Bedside
- (History) Take a full history including effects on life and functional status
- (Observations) Full set of observations, lying and standing blood pressure
- (Corresponding examination) Perform a cerebellar examination
Eye movements – Assess eye movements for progressive supranuclear palsy (PSP)
Cognition – Perform a cognitive assessment (MMSE)
Imaging – DaT Scan
Sources
Gait Cycle – Ducky2315, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Hypomimia – Paul Richer (1849-1933), Public domain, via Wikimedia Commons
Postural Tremor – LuYang’s art works, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Finger Nose Test – https://clinicalgate.com/coordination-2/#F0010
Pronate and Supinate – Mongrangvebet, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Make fist – Free from Pixabay, no attribution required, Pixabay License
Opposition – Connexions, CC BY 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons
Toe Tapping – BruceBlaus, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Micrographia – Jean-Martin Charcot, Public domain, via Wikimedia Commons
Disclaimer
The intended purpose of this website is to be used as a resource for revision for exams. It should not be used as a guideline or reference for clinical practice/decision making or by patients looking for medical information or advice. In2Med takes no responsibility for any loss or damaged resulting from the use of information from this website.


