
































































GALS examination
Click the button to download our free OSCE Book
Introduction
- Wash Your hands
- Introduce yourself by name and role
- Check the patient’s identity – name and Date of Birth
- Explain the procedure – why you need to do it and what does it involve
- Ask for consent
- Expose the patient appropriately
- Check if the patient is currently in any pain
How to Introduce Yourself
“Good morning, my name is .. and I am a medical student. Can I just check your name and date of birth?
I have been asked to do an examination of your muscles and joints today. This will involve asking you to walk and then doing a variety of movements with you arms and legs. Is that ok?
– For the purposes of this examination would you mind removing your gown but keeping your underwear on?
– And before I start, can I just check whether you are in any pain?”
Bedside Inspection
- Observe the patient by standing at the end of the bed.
- Comment on whether the patient is ABC:
A – Alert B – (normal) Body habitus C – Comfortable at rest
- Observe the surroundings and comment about objects of note
Describe the objects or items around a patient’s bedside that will give you an idea into the condition that they might have. It is important to highlight this to the examiner as this can give you many clues about the patient’s underlying diagnosis. Things to look for include
- Medication – can you see any medication on the patient’s bedside e.g. pain relief?
- Mobility aids – gives an idea about the functional status of the patient.
Screening Questions
Question 1:
“Do you have any pain or stiffness in your joints, muscles or your back?”
This question screens for one of the most common symptoms of MSK disease which is pain. You can use this question to see if the pain is generalised or focussed on one particular area. This helps establish the pattern of disease as certain pathologies give specific patterns of pain and stiffness.
Question 2:
“Can you dress yourself without any difficulty?”
This question screens for an impairment in the functional status of the patient. This gives an indication of their severity of disease.
Question 3:
“Do you have any difficulty when going up and down the stairs?”
This question screens for general mobility issues and and impairment in the motor function. This is another key question in establishing the baseline functional status of the patient and what level of intervention then might require.
Gait
Action: Ask the patient to walk to the end of the room, turn around and then walk back.
Assess for:
–> Smoothness: Is there any disruption to the normal gait cycle such as abnormalities in toe-off or heel strike?
–> Symmetry: Is the gait symmetrical on both sides? Asymmetry of the gait could be caused by problems such as leg-length discrepancy, fixed flexion deformity, or pain on one side which reduces full extension and weight bearing on that side.
–> Step Height: A damage to the common fibular nerve for example leads to a foot-drop on the affected side. This means the patient will not be able to dorsiflex which gives them a high step height to compensate.
Types of Gait
The gait cycle is made up of 6 phases.
- Heel-strike: this is when the heel first touches the floor.
- Foot flat: here the weight is transferred onto the leg as the foot is all in contact with the floor.
- Mid-stance: the weight is aligned and balanced on this leg.
- Heel-off: here the heel lifts off as you start to transfer weight onto the other leg.
- Toe-off: this is when the toes finally lift off the floor
- Swing: the foot swings forward until the heel comes back in contact with the ground restarting the cycle.
a) Antalgic gait – a type of gait where the stance phase is abnormally shortened to reduce time on that foot. It looks like a limp –> Implies pain in that leg
b) Waddling gait – this is due to weakness of the proximal muscles of pelvis which causes weakness of gluteus muscles. Patient moves upper body forwards and drags lower leg forward.
c) Spastic gait – this is described as a swinging gait where the patient swings his leg round as it is hyperextended. This is seen in UMN lesions such as stroke
d) High-stepping gait – this is due to damage of the deep branch of the common fibular nerve which leads to foot-drop due to loss of dorsiflexion. This means the patient has a high step in order to compensate.
e) Trendelenburg gait – this leads to dropping of the pelvis on the contralateral side when you are walking. It is due to damage to the gluteus medius on the supported side –> indicates a lesion of the superior gluteal nerve
Observation
Action: Ask the patient to stand upright with their arms by their side. Observe them from the front, side and back for any signs of musculoskeletal disease.
FROM THE FRONT:
Assess for:
–> Posture: See if the patient is hunched over, which may indicate a problem with their spine.
–> Shoulders: Assess the shoulder bulk and whether there is any asymmetry in the muscle bulk of the shoulders.
–> Leg Length: See if there is a discrepancy in the leg lengths. This could be due to joint disease as a child, or a fixed flexion deformity of one of the limbs.
–> Quadriceps: Assess for any wasting of the quadriceps muscle bulk implying damage to the femoral nerve.
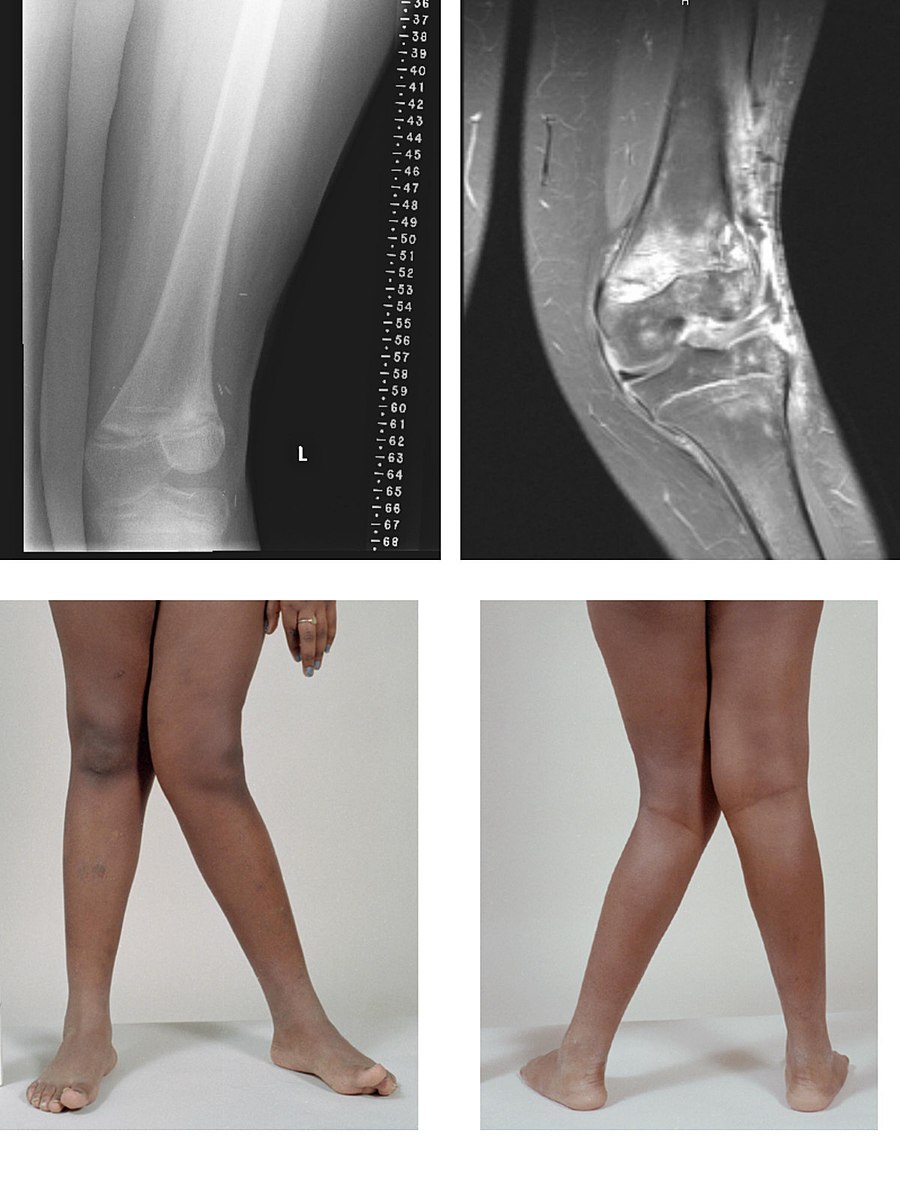
–> Knee: Assess for any obvious swelling or varus/valgus deformity of the knees. Osteoarthritis typically gives a varus deformity whereas rheumatoid gives a valgus deformity.
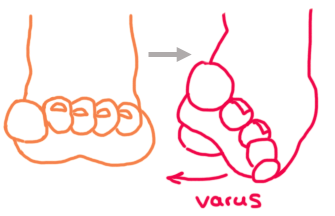
–> Feet: Observe for any bunions (valgus deformity of the great toe)



FROM THE SIDE:
Assess for:
–> Cervical Spine: Check for hyperlordosis of the cervical spine. This is seen in discitis, osteoporosis and spondylolithiesis.
–> Kyphosis/Lordosis: The spine has natural curves but these terms describe when the curves become excessive. This is seen in degenerative conditions which affect the spine.
–> Foot arches: Flattening of the feet or high arched feet are associated with condition. A high arch (pes cavus) is seen in Charcot-Marie-Tooth disease. Flat feet (pes planus) are risk factors for joint problems.
–> Toe clawing: This sign may indicate plantar fiscial fibromatosis.
FROM THE BACK:
Assess for:
–> Shoulders: Pain in the shoulder can also be due to referred pain from internal organs. One differential could be subacute bacterial endocarditis, but only once other more common diagnoses are ruled out.
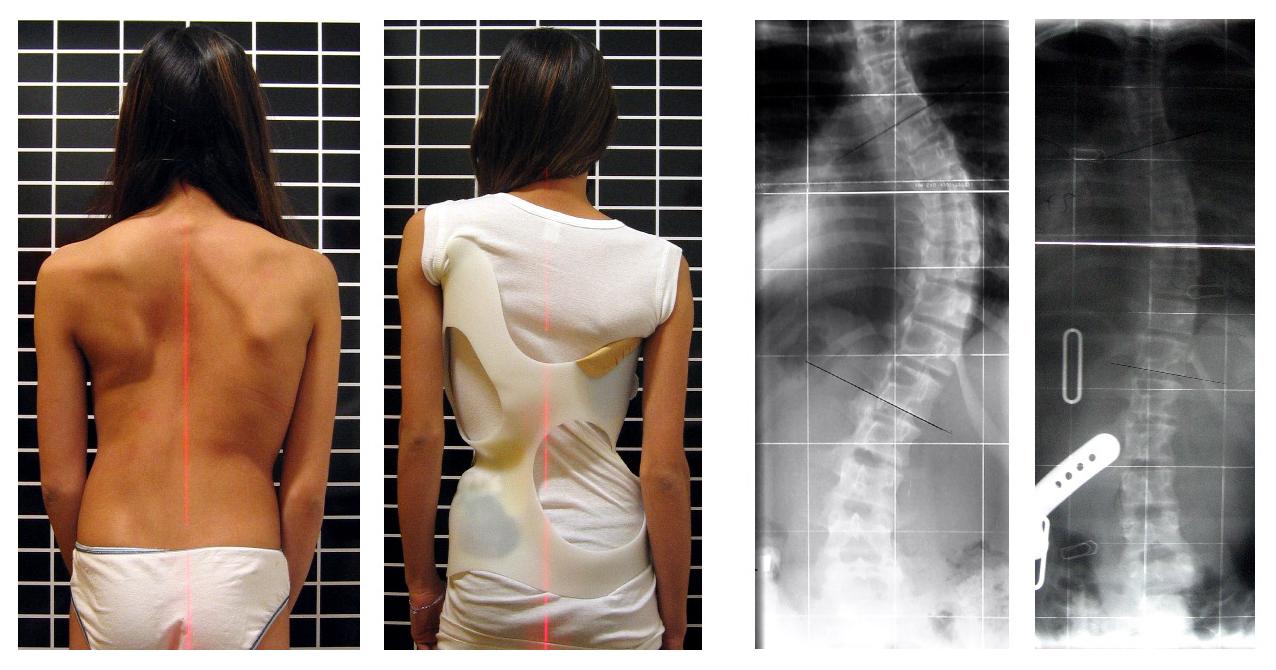
–> Scoliosis: This is a lateral curvature of the spine which is more common in adolescent girls. If severe, this may require surgery to correct the spine.
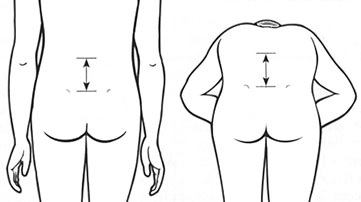
–> Iliac crest: This should be level. Assess this for any pelvic tilt which may indicate weakness of the abductor muscles e.g. gluteus medius.
–> Popliteal fossa: Check the fossa for a Baker’s cyst (non-pulsatile) or a popliteal artery aneurysm.


Spine
Action: Assess lateral flexion by asking the patient to tilt their head from side to side, moving their ears to their shoulders.
Assess for:
–> Lateral flexion of cervical spine: Reduced flexion of the cervical spine could be a sign of ankylosing spondylitis which leads to flexion of the spine. It could also be muscular due to spasms of the trapezius or SCM muscle.
Action: Ask the patient to open their mouth and place the fingers inside their mouth.
Assess for:
–> TMJ joint: Restricted jaw opening could be a sign of temporomandibular joint disease.
Action: Place 2 fingers on the patient’s lumbar vertebrae about 5cm apart. Ask the patient to bend forwards and touch their toes.
Assess for:
–> Schober’s Test: This is a measure of the mobility in the lumbar spine. As the patient leans forward your fingers should move apart.
– If movement is restricted, this suggests reduced lumbar spine movement. It is a sign of Ankylosing Spondylitis
– If the patient is able to fully place both hands on the floor flat, this indicates hypermobility.

Arms
MOVEMENT 1:
Action: Ask the patient to sit down on the couch and put their hands behind their head.
Assess for:
–> Ease of movement: This is a screening movement which in one can assess for shoulder abduction, external rotation and elbow flexion. This gives a general impression of the functional status of the main muscle groups in the arms.

MOVEMENT 2:
Action: Ask patient to hold hands out, palms down and fingers outstretched. This movement is a screening movement which texts the extension of muscle groups in the upper limb.
– In this position closely inspect the backs of the hands and the nails.
– Whilst the patient is in this position, you can lightly squeeze across their metacarpophalangeal joints and see if you can detect any signs of potential discomfort
Assess for:
–> Asymmetry, joint swelling and deformity: These are the hallmarks of any inflammatory joint disease such as psoriatic arthritis/rheumatoid. Mention any particular deformities you find.
–> Nail Changes: Psoriatic arthritis is associated with onycholysis (where the nails come off) and nail pitting.

MOVEMENT 3:
Action: Ask patient to turn hands over so that their palms are facing up and to keep their arms outstretched.
– In this position assess the muscle bulk of the thenar and the hypothenar eminence
Assess for:
–> Muscle wasting: Damage to the media nerve will cause wasting of the muscles in the thenar eminance, which could be due to carpal tunnel syndrome.
MOVEMENT 4:
Action: Ask patient to make a fist with their hands.
Assess for:
–> Flexion of the fingers: This movement assesses flexion of the small joints of the fingers as well as overall hand function.
– If the patient has significant joint swelling or deformity they will be unable to make a fist.
MOVEMENT 5:
Action: Place 2 fingers in your hands patient’s hands and ask them to squeeze your fingers as hard as they can.
Assess for:
–> Power grip: The grip strength can be reduced by many factors e.g. pain (due to inflammatory), swelling (physical restriction) or muscle wasting (damage to nerves)
MOVEMENT 6:
Action: Ask the patient to touch each finger to their thumb in turn, known as the “precision grip”.
Assess for:
–> Precision Grip: This test assesses for coordination of the small muscles of the hand.
– This can be affected by inflammation which reduced intrinsic mobility, or a higher order nervous lesions e.g. cerebellar disease.




Legs
Action: Ask the patient to lie down on the couch and keep their legs outstretched.
– With the backs of your hands, feel the patients legs bilaterally on the medial and lateral sides, seeing if you can find a temperature difference between the two legs.
Assess for:
–> Temperature: A raised temperature is indicative of an inflammatory process occurring. This could be due to an inflammatory arthritis e.g. rheumatoid arthritis, septic arthritis.
Action: Perform a patellar tap test to see if you can detect the presence of an effusion.
a. With the patient’s knee extended, slide your left hand down the thigh to the upper border of the patella. This pushes any potential synovial fluid from the suprapatellar pouch behind the patella.
b. Keep your left hand there and then use your right hand to push downwards on the patella
c. If there is fluid present you will feel a tap as the patella bumps against the femur.
Assess for:
–> Joint Effusion: This test is used to assess for a joint effusion. This is caused by an inflammatory process in the knee joint which can occur for a variety of reasons. These include trauma (e.g. damage to the ligaments), osteoarthritis, or an inflammatory arthritis like rheumatoid or infection (septic arthritis).

Action: Whilst supporting the patient’s leg, flex the knee as far as you are able, making sure to observe for signs of discomfort.
– Whilst doing this, place one hand over the knee joint to see if you can feel any crepitus.
Assess for:
–> Passive Knee Flexion: The normal range of movement is up to 140 degrees. Any joint pathology may reduce this range of motion. It is important to document the range of motion in degrees and whether you can feel any crepitus (crackling) in the joint.

Action: Whilst you are flexing the knee, flex the patient’s hip and knee joint to 90° and then rotate their foot laterally.
Assess for:
–> Passive Internal Hip Rotation: Internal rotation of the hip is one of the first movements to be affected in hip pathologies. Document the range of motion in degrees and whether you can feel any crepitus in the joint. Normal range of motion is 40 degrees.
Action: Gently squeeze across the metatarsophalangeal (MTP) joints and observe for verbal and non-verbal signs of discomfort.
Assess for:
–> Pain/discomfort: This is indicative of an inflammatory process in these joints. This is associated with an inflammatory arthritis such as rheumatoid. Remember, this affects both the hands and feet.
Thank the patient and wash your hands to complete the examination!
On Completion
You must remember that the physical examination is only one part of the overall assessment of your patient. Therefore, when completing your exam, state that you would do the following in order to complete your assessment of the patient. Much of this will depend on whether you have discovered any particular findings or have an idea about the overall diagnosis. However, some essential things to talk about are:
“To complete the examination, I would do a number of steps…”
Bedside:
- (History) Take a full history
- (Observations) Full Obs chart including blood pressure
- (Corresponding examination) Conduct an examination of one of the main joints (where the problem is)
- (Bedside tests) Formally assess grip strength
Bloods – Would take a full blood count, inflammatory markers including ESR + CRP, rheumatoid factor
Imaging – X-ray of one of the joints
Special tests – MRI (if required)
How to Present Your Findings
“I conducted a GALS examination on … who seemed well and comfortable at rest.
- On inspection there were no peripheral signs or paraphernalia of MSK disease
- The gait was smooth with a normal swing and stance phase
- There was normal range of motion in the spine and Schober’s test was negative
- There was normal range of motion in the arms and hands
- There was normal range of motion in the legs and no tenderness
In summary, this is a normal examination.”
Sources
Gait Cycle – Ducky2315, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Knee Effusion – James Heilman, MD, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Valgus Knee Deformity – BioMed Central, CC BY 2.0 <https://creativecommons.org/licenses/by/2.0>, via Wikimedia Commons
Varus Deformity – Ellen L Tsay, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Pelvic Tilt – See page for author, CC BY 2.0 <https://creativecommons.org/licenses/by/2.0>, via Wikimedia Commons
Hallux Valgus – Angela Simon, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Pes Planus – Hellerhoff, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Pes Cavus – Benefros at English Wikipedia, CC BY-SA 3.0 <http://creativecommons.org/licenses/by-sa/3.0/>, via Wikimedia Commons
Scoliosis – Weiss HR, CC BY 2.0 <https://creativecommons.org/licenses/by/2.0>, via Wikimedia Commons
Schober Test – Nasch92, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
TMJ Joint – MathieuMD, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Hands Behind Head – https://openclipart.org/detail/226079/man-relaxing-with-hands-behind-head-silhouette-with-background
Hands In Front – https://www.freepik.com/free-photo/guy-yellow-t-shirt-stretching-arms-forward_7608096.htm
Carpal Tunnel Syndrome – Dr. Harry Gouvas, MD, PhD, Public domain, via Wikimedia Commons
Boutonniere Deformity – Alborz Fallah, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Swan-Neck Deformity – User:Phoenix119, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Dupuytren’s contracture – Frank C. Müller, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Knee ROM -MilitaryDisability(militarydisabilitymadeeasy.com/images/knee/knee%20flexion%201)
Disclaimer
The intended purpose of this website is to be used as a resource for revision for exams. It should not be used as a guideline or reference for clinical practice/decision making or by patients looking for medical information or advice. In2Med takes no responsibility for any loss or damaged resulting from the use of information from this website.


