
































































Cranial Nerve Examination
Click the button to download our free OSCE Book
Introduction
- Wash Your hands
- Introduce yourself by name and Role
- Check the patient’s identity – name and Date of Birth
- Explain the procedure – why you need to do it and what does it involve
- Ask for consent
- Expose the patient appropriately
- Check if the patient is currently in any pain
- Ask if they are right or left-handed
How to Introduce Yourself
“Good morning, my name is .. and I am a medical student. Can I just check your name and date of birth?
I have been asked to do an examination of the nerves supplying your head and neck. This will involve me testing your vision and hearing, as well as the movement and sensation in your face and neck. Is that ok?
– Before I start, can I just check whether you are in any pain?”
Bedside Inspection
- Observe the patient: Patient is A – Alert B – (normal) Body habitus C – Comfortable at rest
- Look for any gross abormalities – limb position, pupils, facial asymmetry
- Observe the surroundings: mobility aids (wheelchair, walking stick), glasses, medication, hearing aids
Cranial Nerve I (Olfactory)
The olfactory nerve transmits information about smell from the nasal epithelium to the brain and so it is a purely sensory nerve. In a cranial nerve examination, we test this by asking about the patient’s sense of smell.
Action: Ask the patient if they have notices a change in smell recently
Assess for:
–> Changes in smell: You need to assess whether this is an acute change or whether it is chronic. Has the patient ever had a sense of smell? And then also ask what might have occurred to cause this e.g. trauma to the nose?
You can also formally assess the sense of smell. It is unlikely you will have time to do this in an OSCE, but you can say to your examiner that you would do this if you had more time.
Action: Use a scented bottle (e.g. coffee/mint) and ask the patient to close their eyes. Place the scent near their nostril and ask them to name the smell. You must test each nostril individually.
Cranial Nerve II (optic)
The optic nerve is purely a sensory nerve, which carries visual information from the retina to the occipital cortex of the brain. There are many different things to assess when examining the optic nerve, including acuity, colour vision, fields, reflexes etc. To make it easier to remember, learn it in 3 groups of 3 (3×3).
1. Acuity
Ask the patient if they wear glasses. If they do, then allow them to keep them on during the assessment. You want to assess for any acute changes in acuity, rather a chronic myopia.
Action: Sit opposite the patient facing them. Ask the patient to cover one eye with the palm of their hand. Test the uncovered eye on 3 things and then switch over to test the other eye. :
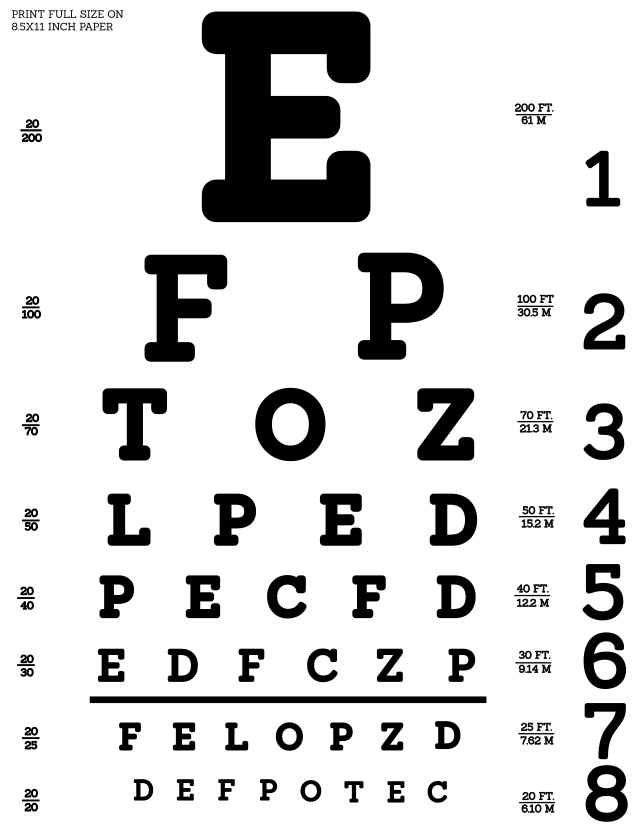
a) Distant vision: Ask the patient to read a line of text behind you. You can also formally assess distant vision using a Snellen chart.
b) Near vision: Ask the patient to read a line of a magazine or a close object like your name badge. If they are unable to do this, ask them to count the number of fingers you are holding up.
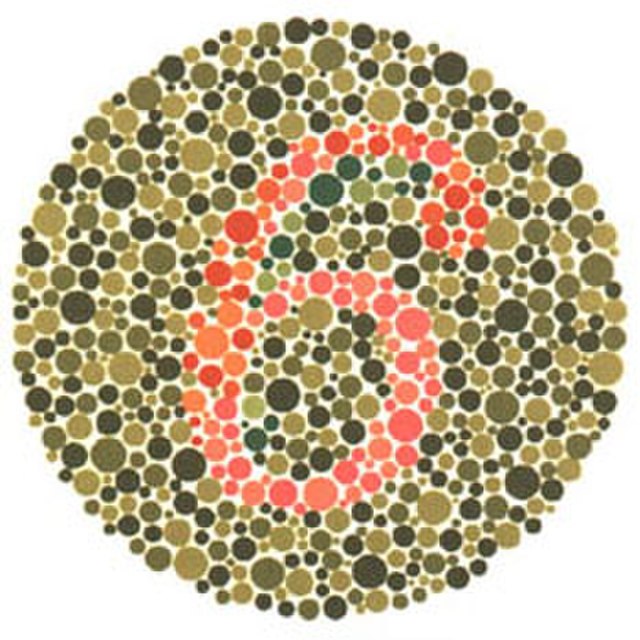
c) Colour vision : Ask the patient to name the colour of a piece of clothing.
Formal tests: Whilst not expected to do this in an OSCE, you should mention that in an ideal setting you would formally assess acuity using a Snellen chart and colour vision using Ishihara plates.
2. Visual Fields
The next set of three involves testing the visual fields.
a) Visual Inattention
Action: Again continue sitting opposite the patient 1m away.
a. Ask the patient to keep both eyes open and focus on looking at your nose.
b. Hold both of your hands out to the side, one in each other patient’s visual field (left and right)
c. Wiggle a finger on each hand and ask the patient to name which hand has moved.
d. To finish, wiggle both fingers at the same time and see if the patient can correctly identify both fingers have moved.
Assess for:
–> Neglect: This is a problem in the awareness of stimuli in one side of their visual field. It is caused by parietal lobe lesions usually after stroke. Inattention to one side = contralateral parietal lesion
b) Visual field mapping
Action: Sit the patient one meter across from you and ask the patient to cover their left eye with their left hand. You should mirror the patient and cover your right eye with your right hand. Tell them to focus their vision on your nose.
a. Using your left hand, put it in the top left of your visual field and start wiggling your fingers.
b. Start to move your hand slowly towards the centre of the visual field.
c. Ask the patient to say “yes” when they can see your fingers moving.
d. Once they say yes, repeat the process in the bottom left quadrant.
e. Once this is done, use your left hand to cover your right eye. Now examine the other side of the patient’s visual field using the same method.
f. Use this to form a map of the patient’s visual field. They should be able to see your fingers when you do.
g. Repeat this process with the other eye.
Assess for:
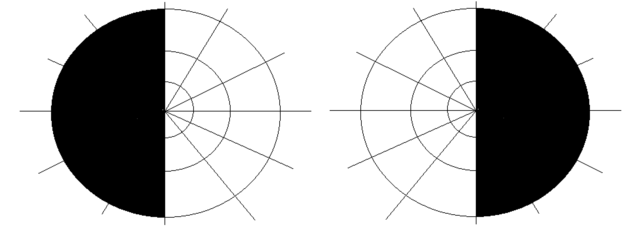
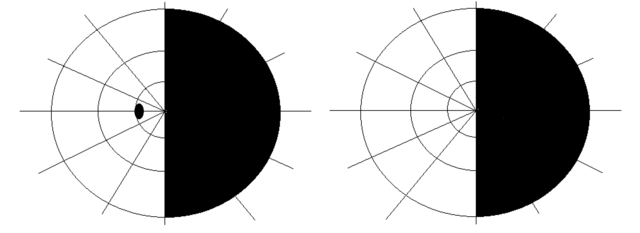
–> Visual field deficits: The patient should say “yes” when you can also see your fingers wiggling. There are different types of visual field loss which indicate optic nerve lesions at various points in the pathway.
c) Blind spot:
Action: Use the same setup as for visual field testing. Cover one eye and ask the patient to focus on your nose.
a. This time, hold a red pin in the periphery of the visual field, horizontal to the midline.
b. Move the pin horizontally from the periphery inwards.
c. Ask the patient to say “yes” when it disappears and then when it reappears
Assess for:
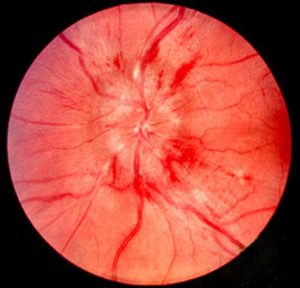
–> Enlarged blind spot: As you are sitting opposite the patient, their blind spot should be the same size as yours. An enlarged blind spot can be due to swelling of the optic disc (papilloedema) which is due to raised intracranial pressure.
Papilloedema
Papilloedema is a potential sign of raised intracranial pressure. This can be observed during an opthalmoscopy – a test that can observe the back of the eye in more detail – including the optic disc. Papilloedema is a swollen optic disc and causes the disc to appear irregular and cloudy.
3. Reflexes
The last set of the 3×3 involves testing the eye reflexes.
a) Accommodation:
Action: Sit opposite the patient and ask them to keep both eyes open.
a. Ask the patient to focus on an object behind you e.g. the clock on the wall.
b. Place your finger in the middle of their view but ask them to continue looking at the object behind you
c. Now ask the patient to shift focus onto your finger
d. Move the finger closer to their face and ask them to continue looking at it.
Assess for:
–> Convergence and pupil constriction: In a healthy person, as your finger gets closer, the eyes should converge and the pupils constrict. Place your finger approximately 20-30cm in front of their eyes (alternatively, use the patient’s own thumb).

b) Pupil reflex:
Action: Ask the patient to hold their hand on their nose between their eyes.
a. Shine a light using your pen torch in one eye. Observe what happens to the pupil in that eye.
b. Remove the light source allowing the pupil to reset.
c. Shine a light in the same eye, but this time observe the pupil in the other eye.
d. Repeat these steps with the other eye.
Assess for:
–> Direct pupillary reflex: When shining a light in one eye, the pupil of that eye should constrict. Failure to do so indicates either a problem in the optic nerve of that eye or the occulomotor nerve.
–> Consensual pupillary reflex: In a healthy person, shining a light in one eye should cause pupillary constriction of both eyes. This is because the optic nerve sends information to both Edinger-Westphal nuclei which innervates both eyes.
c) Swinging Light test:
Action: Tell the patient to remove their hand from between their eyes.
a. Shine a light into one eye.
b. Rapidly swing the light shining the light into each eye one by one.
Assess for:
–> Marcus-Gunn Pupil: This is a relative afferent pupillary defect.
In a healthy person, when light is shined into either eye, both pupils should constrict by the same amount.
– If there is a problem with the optic nerve of one eye, this means it detects less light shining on the eye and transmits less sensory info. Therefore, the pupils will constrict less and the brain thinks it is dimmer.
– So, in the swinging light test, you will see that shining a light into one eye causes more constriction than shining it into the other.
– Another way of seeing this, is that when switching light from good eye to the bad eye, the pupils will actually dilate, as the brain thinks the light source is becoming dimmer.
Once you have completed the 3×3 tests, mention that you would formally assess the eyes using fundoscopy.
Fundoscopy
Firstly prepare the patient by introducing what you are going to be doing and gain informed consent.
Inspect the eye and the skin around the eye for any abnormalities. Check the size and shape of the pupils.
To inspect the optic disc, it may be useful to administer some mydriatic eye drops to help dilate the pupil, then dim the lights to create a darker environment. Ask the patient to stare straight ahead and keep their eyes open.
Turn the opthalmascope on and adjust the light setting. If you are inspecting the patient’s right eye then place your left hand on the patient’s forehead and hold the opthalmascope in your right hand to prevent you from colliding with the patient.
Approach the patient from a 10/ 15 degree angle and observe the ‘red reflex’. When you are appropriately close to the patient, increase the resolution of the opthalmascope to observe the blood vessels at the back of the retina. Follow these medially to locate the optic disc.
Cranial nerve III (Oculomotor), IV (Trochlear), VI (Abducens)
These 3 nerves are responsible for controlling eye movements.
– CN III – This gives innervation to medial, superior and inferior rectus, inferior oblique and levator palpebrae superioris. It also gives parasympathetic innervation to the eye responsible for pupillary constriction.
– CN IV – This innervates superior oblique which abducts and moves the eyeball inferiorly
– CN VI – This innervates lateral rectus which abducts the eye.
Therefore, to test these nerves, we examine the eye movements of the patient.
INSPECTION
Action: Ask the patient to look directly at you.
Assess for:
–> Ptosis : This is a sign defined by drooping of the eyelids. Full ptosis is seen in an occulomotor nerve lesion, whereas partial ptosis is seen in Horner’s syndrome due to disruption of sympathetic fibres.
–>Strabismus/squint: This is a misalignment of the eyes. It may manifest itself as the patient’s eyes pointing in opposite directions or a misalignment.


MOTOR
Action: Perform the H-test to assess the motor function of the extra-ocular muscles.
a. Sit opposite the patient and hold your finger up in front of the patient’s eyes. Ask the patient to focus on your finger.
b. You can use your other hand to support the top of the patient’s head to ensure that the head stays still.
c. Ask the patient to follow your finger with their eyes, ensuring they keep their head still.
d. Move your finger from side to side, then up and down creating a big “H” pattern.
Assess for:
–> Double vision: Ask the patient to mention when they get double vision. This could be caused by paralysis of one of the extra-ocular muscles. Find which direction the patient experiences double vision in.
–> Nystagmus: This is an involuntary rhythmic side-to-side, up and down or circular motion of the eyes that occurs with a variety of conditions, which includes cerebellar disease, stroke or vestibular nerve dysfunction.
–> Complex opthalmoplegia: This is many abnormal eye movements which do not fit single nerve lesion. This is due to more conditions which affect multiple nerves like myasthenia gravis or brainstem lesion.
CN III, IV and VI nerve palsies
CN III Palsy:
– This results in paralysis of most of the extraocular muscles, except lateral recuts and superior oblique. Therefore, this means the eyeball is pulled “down and out”.
– In addition, there is damage to the parasympathetic fibres which leads to ptosis (due to paralysis of levator palpebrae superioris) and a dilated pupil (due to loss of innervation to sphincter pupillae). CN III is a serious sign and it is seen in raised intracranial pressure which causes uncal hernation (this is a stage before death)
CN IV Palsy:
– This leads to paralysis of superior oblique, which is responsible for depressing and abducting the eye.
– Therefore, this gives vertical diplopia when looking down. The eyeball will be unable to adduct and then look down.
CN VI Palsy:
– This leads to paralysis of lateral rectus which abducts the eye. Therefore this means the eyeball will be unable to look laterally and will look medially at rest due to the unopposed action of medial rectus. CN VI is the first nerve affected in raised intracranial pressure.
Action: If you suspect that strabismus is present, you should offer to do the cover test to characterise it.
a. Ask the patient to focus on an object.
b. Cover one of the patient’s eyes and observe the other eye.
Assess for:
–> Shift in fixation: If the uncovered eye shifts fixation, this indicates that the eyes were misaligned. This is seen as the eye has now corrected once the stimulus from the other eye is covered. If there is no change, then this shows the eyes were aligned.
Cranial nerve V (Trigeminal)
The trigeminal nerve has both sensory and motor components. It supplies sensations to the face and neck as well as motor innervation to the muscles of mastication (eating). It is made up of 3 main branches:
– Va (opthalmic) – gives rise to frontal, lacrimal and nasociliary branches. Carries sensory information scalp and forehead, nose, upper eyelid and conjunctiva of eye.
– Vb (maxillary) – gives zygomatic, buccal and infraganglionic branches. Carries sensory information from lower eyelid, cheek, nares, upper lip, upper teeth and gums.
– Vc (mandibular) – innervates the muscles of mastication. Also carries sensory information from, jaw, lower lip, bottom row of teeth and chin.
Therefore, in order to test the trigeminal nerve function, we assess the sensation of the face and motor functions of the muscles of mastication.
SENSATION
With sensation, you want to characterise the distribution of sensory changes and compare side to side.
You will also want to test different modalities, but for the purposes of your OSCE, you should assess light touch.
Action: Test the sense of light touch using a piece of cotton wool (or lightly tapping)
a. Ask the patient to close their eyes and brush the cotton wool on their sternum. Explain that this is what it will feel like
b. Tell the patient that you will tap them lightly. Ask them to say “Yes” when they can feel something.
c. Brush the cotton wool in the following areas, which are supplied by particular nerves. For each dermatome, compare side by side, and ask “Does it feel the same on both sides”
| Lateral forehead | Opthalmic Nerve (Va) |
| Lateral cheek | Maxillary Nerve (Vb) |
| Lateral chin | Mandibular Nerve (Vc) |
MOTOR
Action: Ask the patient to look at you. Observe their face closely.
Assess for:
–> Wasting: Damage to CN V will cause wasting of the temporalis and masseter muscles.

Action: Assess the power of the muscles of mastication:
a. Ask the patient to clench their mouth shut. Feel for the muscle bulk in the temporalis fossa and the bulk of the masseter muscle.
b. Next, place your hand under the patient’s mouth and ask the patient to open their mouth against the resistance of your hand.
Assess for:
–> Muscle weakness: A trigeminal nerve palsy leads to weakness of the lateral pterygoids, which are the muscles which open the mouth.
–> Jaw deviation: A trigeminal nerve palsy will cause jaw deviation towards the side of the lesion.
REFLEXES
Action: Offer to test for the corneal reflex and jaw jerk reflex. It is unlikely you will be asked to do this in your OSCE, but you should offer to test it and understand the physiology behind the tests.
Corneal Reflex
This is a reflex that tests the function of cranial nerves V (trigeminal) and VII (facial) nerves. It tests the ability of the body to blink in response to stimulation of the cornea. This is a protective feature which closes the eyes if a dangerous stimulus comes close to the eye.
Normally, when a stimulus touches the cornea, this is detected by the sensory fibres of Va (opthalmic nerve).
– This impulse then travels to the brain
– It then innervates both facial nerve nuclei
– The impulse is then carried down the efferent branch which is mediated by the temporal and zygomatic branches of the facial nerve (CN VII).
To test the reflex:
– Using cotton wool, slowly touch the edge of the cornea. It is important to approach from the side as you don’t want the patient to blink as they see you. This would be testing the optic nerve.
Assess for:
–> Direct and consensual blinking: Failure to blink means either a problem in Va (sensory) or in the facial nerve (motor).
Cranial nerve VII (facial)
The facial nerve has many functions which we can assess in the cranial nerve examination:
– Motor: Supplies the muscles of facial expression
– Sensory: Somatic fibres to the external ear and tympanic membrane
– Special Sensory: Taste of the anterior 2/3rds of the tongue
– Autonomic: Parasympathetic fibres to the submandibular and sublingual gland
As it can be difficult to assess all of these, in the cranial nerve examination, we focus on assessing the motor and special sensory components of the facial nerve. One of the main goals in facial nerve testing is to be able to differentiate stroke vs Bell’s Palsy.
Muscles of Facial Expression
Action: Take a look at the face and observe for any irregularities in the muscles:
Assess for:
–> Face asymmetry: Damage to the facial nerve leads to iplilateral facial paralysis. This will give the patient a drooped face on one side. Look particularly at the mouth (smile) and nasolabial fold
–> Wrinkles of the forehead: If a patient cannot wrinkle their forehead, this indicates a LMN lesion to the facial nerve. In stroke, forehead wrinkling is preserved.

Action: Ask the patient to make a series of specific movements to assess the motor function of their facial muscles.
– After they have made the movement ask them to hold the expression whilst you try and oppose the movement:
a. Ask patient to raise up their eyebrows and not let you push them down- Assesses frontalis (temporal branch)
b. Ask patient to scrunch up their eyes and don’t let you open them – Assesses orbicularis oculi (zygomatic branch)
c. Ask them to puff their cheeks out and don’t let you push them in – Assesses buccinator (buccal branch)
d. Ask patient to smile showing their teeth – Assesses orbicularis oris (mandibular branch)
e. Ask patient to grimace – Assesses platysma (cervical branch)
Differentiating Stroke and Bell's Palsy
Stroke and Bell’s palsy can present very similarly, as they can both lead to facial paralysis on one side. One of the key ways to differentiate between them is by assessing whether the patient can wrinkle their eyebrows.
– In Bell’s palsy, the whole of the facial nerve is affected, including the frontal branch which innervates frontalis. This means that the patient loses innervation of this muscle and so they cannot raise their eyebrows or wrinkle their forehead.
– In a stroke, the problem is in the central nervous system. A blot clot causes ischaemia and damage to the part of the brain which innervates the facial nerve nucleus. However, the top of the of the facial nerve nucleus received bilateral innervation from both hemispheres.
This means that is a stroke, the top part of the facial nerve nucleus can still get innervation from the part of the brain not affected by the stroke. This means the frontal branch is still intact and can innervate the frontalis muscle so the patient can raise their eyebrows.
In a full CN exam, there will also be other features which help delineate between Bell’s palsy and stroke e.g. aphasia, visual symptoms etc. But this often comes up in medical exams so be sure to learn it.
STAPEDIUS
Action: Ask the patient if they have found that sounds are sounding abnormally loud
Assess for:
–> Hyperacusis: This is a sensation where sounds appear abnormally loud. This can be due to damage to stapedius which is a muscle in the middle ear that helps to dampen sound. If this is present, it indicates that the lesion to the facial nerve is more proximal, before it has split into its 5 motor branches in the parotid gland.
-Offer to check taste sensation over anterior 2/3 of the tongue (chorda tympani)
TASTE
Action: Ask the patient if they have notice any changes in their taste
Assess for:
–> Changes of taste: If the patient answers yes to this question, you can offer to formally assess taste sensation by asking the patient to identify different flavours. It is unlikely you will be asked to do this in an OSCE but it is good to be aware of it.
Cranial Nerve VIII (Vestibulocochlear)
The vestibulocochlear nerve is a purely sensory nerve which carries sensory information regarding hearing and balance. Therefore, in order to test this, we need to assess the patient’s hearing and sense of balance.
To start, ask the patient whether they have noticed any abnormalities in hearing (e.g. tinnitus) or balance (vertigo).
Hearing
There are 3 tests that we use to assess hearing.
1. Crude hearing test:
Action: Assess the patient’s general sense of hearing in each ear.
a. Tell the patient that you are going to whisper a word in their ear and that they need to repeat it back to you.
b. Go close to the patient’s right ear. As you do so, mask the other ear which is not being tested by rubbing the tragus.
c. Whisper a word into the ear being tested and ask them to say it out loud.
d. If they do not hear, try again speaking louder.
e. Once complete, test the other ear in the same way.
Assess for:
–> Hearing loss: Assess if there is a deficit in hearing in one of the ears. If you find there is an issue in one, or even both ears, you can then assess whether there is a sensorineural or conductive hearing loss.
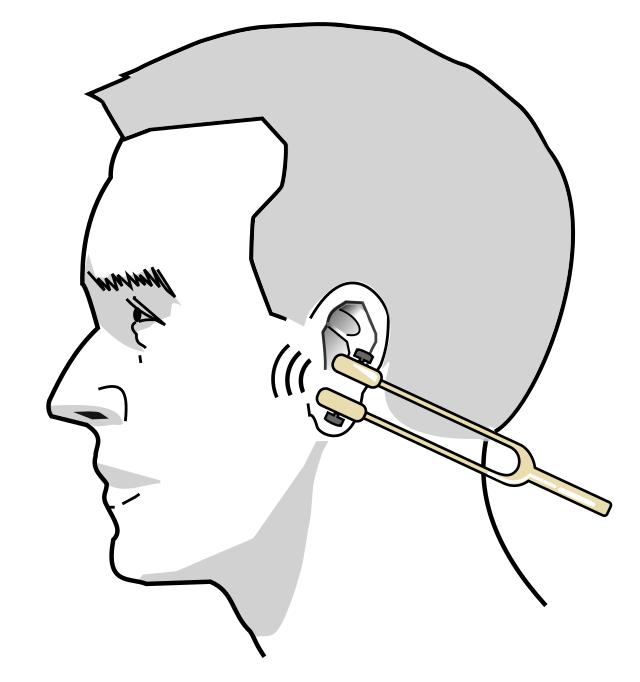
2. Weber’s Test
Action: Perform Weber’s test:
a. Using a 512Hz tuning fork, tap it against your knee so it starts vibrating.
b. Place the tuning fork on the middle of the patient’s forehead and ask them “which ear do you hear the sound loudest in.”
Assess for:
–> Unequal sound volume: In a healthy person, the sound should be equally loud in both ears.
– If one side is louder, this means either that side has a conductive hearing loss, or the other side has a sensorineural hearing deficit.

3. Rinne’s Test
Action: Perform Rinne’s test:
a. Using a 512Hz tuning fork, tap it against your knee so it starts vibrating.
b. Then place the base of the tuning fork against the patient’s mastoid process of their right ear. Keep it there for 2 seconds to let them hear the intensity of the sound.
c. Next, lift off the tuning fork and place the vibrating tips about 1cm from their external auditory meatus. Leave it there for a few seconds.
d. Ask the patient in which position they heard the sound loudest
e. Repeat the test on the other ear.
Assess for:
–> Bone vs air conduction: In a healthy person, air conduction is better than bone conduction, so the sound should be loudest when you hold the tuning fork 1cm from the external meatus:
– If air conduction is louder –> This is Rinne’s Positive (no conductive hearing loss on this side)
– If bone conduction is louder –> Rinne’s negative (conductive hearing loss on this side)
You have to use Weber’s test and Rinne’s test together to work out the hearing deficit. Weber’s test tells you that one side has a conductive or sensorineural hearing loss – Rinne’s test identifies if one side has a conductive hearing loss. This means you can diagnose a sensorineural hearing loss by exclusion.
Worked through Example:
Weber’s Test reveals sound in louder on the right side:
– Either there is a conductive hearing deficit in the right ear or
– There is a sensorineural hearing deficit in the left ear.
To distinguish between these, we can use Rinne’s test.
– Rinne’s test shows air conduction louder than bone in right ear. This means this ear is normal
– Shows air conduction louder than bone in left ear too.
This means the patient has left sensorineural hearing loss.
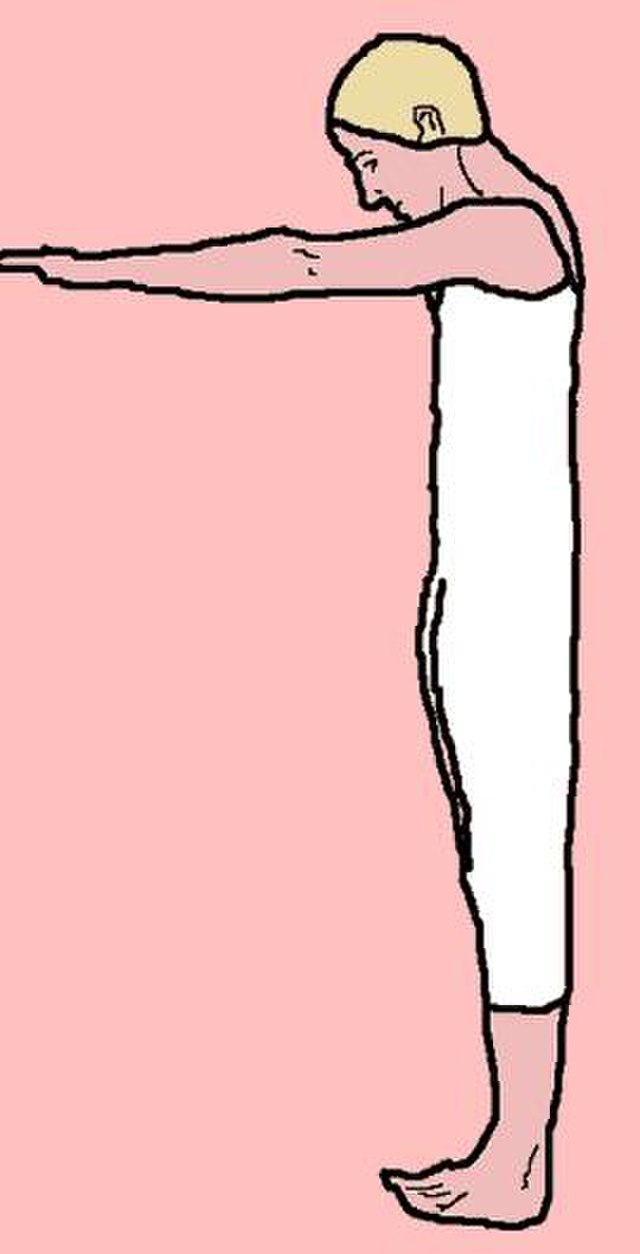
Balance
Balance is coordinated by the cerebellum which receives input from 3 places. Proprioception, vestibular system and vision. You need at least 2 to keep balance. Romberg’s test removes vision leaving the other two, so you can identify whether the issue is with one of these, or the cerebellum itself which cannot integrate the various stimuli.
Action – Perform Romberg’s test of balance.
a. Position yourself within arms reach of the patient to allow you to intervene should they begin to fall.
b. Ask the patient to put their feet together and keep their arms by their sides (be aware that patients with truncal ataxia may struggle to do this, however, this type of unsteadiness is not the same as a positive Romberg’s sign).
c. Ask the patient to close their eyes.
Assess for:
–> Balance – this is a test which can be used to assess whether there is a problem with proprioception, vestibular function or the cerebellum.
– If patient feels unsteady with eyes closed – this is a positive Romberg’s sign. This shows problem is due to sensory problem (due to proprioceptive disorder or vestibular dysfunction) as the patient feels unsteady when the visual stimulus is removed.
– If patient feels unsteady with eyes open – this is a negative Romberg’s sign. This shows problem is in the cerebellum, due to an issues with coordinating the different sensory inputs.
In addition, if you find problems with balance you should offer the Dix-Hallpike test. This is used to assess for benign paroxysmal positional vertigo. In your OSCE, it is unlikely you will be asked to do this, but it is a good test to learn as it is a common presentation in GP.
Also offer inspection of the ears with an auroscope if any of the previous tests are abnormal.
Cranial Nerve IX (Glossopharyngeal) & X (Vagus)
In the cranial nerve exam, we assess IX and X together as they both contribute together to allow different functions.
– CN IX – Covers taste from the posterior 1/3 of the tongue, supplies stylopharyngeus muscle and gives parasympathetic fibres to the parotid gland.
– CN X – Gives sensation of the external ear, the pharynx, larynx and viscera. It carries taste from the epiglottis and viscera and innervates muscles of the pharynx and larynx. It also gives parasympathetic fibres to the neck, thorax and abdomen.
Therefore, to assess these 2 nerves, we assess the mouth, the cough and swallow and the gag reflex.
Mouth
Action: Ask the patient to open their mouth and say “ahh.” Use a pen torch to look inside the mouth.
Assess for:
– Uvula Deviation: The uvula and soft palate muscles are supplied by CN IX and X. In a vagus nerve lesion, the uvula will deviate away from the affected side.

Action: Ask the patient to cough
Assess for:
–> Vagus Nerve lesions: Being able to cough requires you to be able to close the epiglottis, raise intra-abdoninal pressure and contract your muscles against a closed glottis. In a vagus nerve lesion, this will cause a weak, non-forceful cough.
Action: Ask the patient to speak
Assess for:
–> Hoarse voice: The vagus nerve gives rise to the recurrent laryngeal nerve which supplies the larynx. A lesion in this nerve gives rise to a hoarse voice due to paralysis or dysfunction of the vocal cords.
Action: Offer the patient a glass of water and ask them to take a few sips so you can assess their swallow.
Assess for:
–> Poor swallow: In order to swallow, this requires a carefully coordinated movement which relies on sensory fibres of CN IX and efferent motor fibres of CN X which innervate the muscles of the pharynx. Dysfunction to any of these nerve can give rise to a poor, unsafe swallow. This patient is therefore at risk of aspiration and choking.

Action: Offer to test for the gag reflex. In your OSCE it is very unlikely you will be asked to do this, but it is important that you are aware that it can be done.
Gag Reflex
The gag reflex is coordinated by the sensory fibres of CN IX and efferent fibres of CN X. It is an important protective mechanism designed to protect the airway and expel unpleasant components from the pharynx.
To do the rest, stimulate the very posterior part of the tongue and pharynx.
This should result in a reflex gag – in some circumstances the patient could even regurgitate food.
Absence of this reflex is a concerning sign and highlights dysfunction of the cranial nerves.
Cranial Nerve XI (Spinal Accessory Nerve)
The spinal accessory nerve is a motor nerve which does not have a sensory component. It supplies 2 muscles, the sternocleidomastoid and trapezius. Therefore, to test the function of this nerve, we assess the motor function of SCM and trapezius.
Action: Inspect the SCM and trapezius
Assess for:
–> Muscle wasting: This is what happens to muscles when they lose nervous innervation. It is a clinical sign which is usually associated with a lower motor neurone problem. Look especially for plantar foot wasting or dorsal foot guttering.

Action: Place your hands on the patient’s shoulders and apply downwards pressure. Ask the patient to try raise their shoulders against the resistance of your hands
Assess for:
–> Trapezius muscle weakness: Damage to the accessory nerve will cause trapezius muscle weakness. This can be unilateral or bilateral.
Action: Place your hand on the right side of the patients face, and ask them to turn their head right whilst you resist the movement.
Assess for:
–> SCM muscle weakness: Damage to the accessory nerve will cause SCM muscle weakness. This may also result in torticollis.
Cranial Nerve XII (Hypoglossal)
The hypoglossal nerve is a purely motor nerve with no sensory component. It innervates the extrinsic muscles of the tongue including genioglossus, hyoglossus and styloglossus. You therefore test the hypoglossal nerve by testing the movements and power of the tongue.
Action: Ask the patient to open mouth. Using a pen torch have a look at their tongue.
Assess for:
–> Wasting: This is what happens to muscles when they lose nervous innervation. It is a clinical sign which is usually associated with a lower motor neurone problem. Look especially for plantar foot wasting or dorsal foot guttering.
–> Fasciculations: These are tiny contractions of muscle which may look like cramping of the muscle to the naked eye. They are associated with lower motor neurone lesions
Action: Ask patient to stick out tongue and move from side to side
Assess for:
–> Tongue deviation: The hypoglossal nerve innervates genioglossus which is responsible for protuding the tongue. A damage to the hypoglossal nerve means that side of the tongue loses innervation so the tongue does not protude straight. Instead the weight of the muscle causes the tongue to deviate towards the side of the lesion.

Action: Test the power of the tongue muscles:
a. With the patient’s mouth closes place your finger on their cheek
b. Ask the patient to push their tongue against their cheek from the inside and push against your finger
c. Repeat this on the other side.
Assess for:
–> Weakness: A hypoglossal nerve palsy will lead to reduced power on that side.
Bulbar palsy
Bulbar palsy is a cluster of symptoms linked to damage to the Glossopharyngeal (CNIX), Vagus (CNX), Accessory (CNXI) and Hypoglossal nerves (CNXII).
These symptoms include:
- Dysphagia – difficulty swallowing
- Difficulty chewing
- Dysphonia – difficulty speaking
- Muscles atrophy such as in the tongue
- Drooling saliva
- Loss of or absent gag reflex
Some causes of bulbar palsy include strokes and tumours affecting the brainstem –> LMN lesion.
Thank the patient and wash your hands again.
On Completion
“To complete the examination, I would do a number of steps…”
Bedside
- (History) Take a full history including effects on life and functional status
- (Observations) Full set of observations
- (Corresponding examination) Conduct a neurological assessment of upper and lower limbs. Offer a full assessment of cognitive and higher order functions like speech
Bloods – FBC, inflammatory markers, renal profile etc.
Imaging – CT head/MRI scan (if indicated)
Special Tests – Opthalmoscope/hearing test (if indicated)
Sources
Snellen Chart – Khex14, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Ishihara Plates – Wellcome Collection gallery (2018-03-29, CC BY 4.0 <https://creativecommons.org/licenses/by/4.0>, via Wikimedia Commons
Bitemporal Hemianopia – RobertB3009, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Homonymous hemianopia – RobertB3009, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Papilloedema – Jonathan Trobe, M.D. – University of Michigan Kellogg Eye Center, CC BY 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons
Accomodation – MikeRun, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Ptosis – tB, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Squint – Pixabay, no attribution required
Facial Nerve Muscles – Medical illustration of branches of the facial nerve © University of Dundee School of Medicine 2015. Illustrated by Annie Campbell. Attribution-NonCommercial-NoDerivatives Creative Commons licence (CC BY-NC-ND 4.0)
Weber’s Test – DrSaltMD, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Rinne’s Test – FOX 52, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Romberg’s Test – Gonad, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Uvula Deviation – James Heilman,MD, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
Swallowing – Bolus position during deglutition. This work by Cenveo is licensed under a Creative Commons Attribution 3.0 United States (http://creativecommons.org/licenses/by/3.0/us/).
Accessory Nerve Muscles – OpenStax College, CC BY 3.0 <https://creativecommons.org/licenses/by/3.0>, via Wikimedia Commons
Hypoglossal Nerve Palsy – Mukherjee SK, Gowshami CB, Salam A, Kuddus R, Farazi MA, Baksh J, CC BY 2.0 <https://creativecommons.org/licenses/by/2.0>, via Wikimedia Commons
Disclaimer
The intended purpose of this website is to be used as a resource for revision for exams. It should not be used as a guideline or reference for clinical practice/decision making or by patients looking for medical information or advice. In2Med takes no responsibility for any loss or damaged resulting from the use of information from this website.


